CASE PRESENTATION
Mandibular prognathism in a patient with an open bite: A case presentation
Prognatismo mandibular en un paciente con mordida abierta: Presentación de un caso
Ladys Marian Guerra Guasch 1, https://orcid.org/0009-0001-1817-5824
Adriana Mercader Cabeza 1*, https://orcid.org/0009-0003-2825-4256
Maribel Sardiña Valdés 1, https://orcid.org/0000-0002-2083-4075
Ivette Pérez Pereira 1, https://orcid.org/0000-0003-0527-2534
1 University of Medical Sciences of Matanzas. Faculty of Medical Sciences of Matanzas “Dr. Juan Guiteras Gener”. Matanzas, Cuba.
* Corresponding Author: adryamc88@gmail.com
Received: 17/08/2025
Accepted: 15/12/2025
How to cite this article: Guerra-Guasch LM; Mercader-Cabeza A; Sardiña-Valdés M; Pérez-Pereira I. Mandibular prognathism in a patient with an open bite: A case presentation. MedEst. [Internet]. 2025 [cited access date]; 5:e472. Available in: https://revmedest.sld.cu/index.php/medest/article/view/472
ABSTRACT
Introduction: dentomaxillofacial deformities, such as the combination of mandibular prognathism and anterior open bite, present a complex clinical challenge due to their multifaceted impact on stomatognathic function, facial aesthetics, and the patient's psychosocial well-being. Successful treatment at the end of growth requires accurate diagnosis and a coordinated approach between orthodontics and maxillofacial surgery to achieve stable and satisfactory results.
Objective: to describe the diagnostic-therapeutic approach and the results obtained after combined orthodontic-surgical treatment in a patient with severe mandibular prognathism and anterior open bite.
Case presentation: an 18-year-old male patient with a family history of prognathism presented with aesthetic and functional concerns. Clinical examination revealed increased lower facial third, lip incompetence, right mandibular deviation, bilateral Class III molar relationship, a -6 mm overjet, and a 2.7 mm anterior open bite. Cephalometric analysis confirmed the diagnosis of severe skeletal discrepancy (anb = -6°). Treatment consisted of a pre-surgical orthodontic decompensation phase, followed by bimaxillary surgery and a final orthodontic phase of occlusal detailing.
Conclusions: integrated orthodontic-surgical management effectively corrected this complex skeletal deformity. A stable Class I occlusion was achieved, the open bite was eliminated, and facial harmony was significantly improved. This case highlights the crucial importance of multidisciplinary teamwork and sequential planning to simultaneously address function and esthetics, positively impacting the patient's quality of life.
Keywords: Mandibular prognathism; Open bite; Orthognathic surgery; Orthodontics; Skeletal Class III
RESUMEN
Introducción: las deformidades dentomaxilofaciales, como la combinación de prognatismo mandibular y mordida abierta anterior, representan un desafío clínico complejo debido a su impacto multifacético en la función estomatognática, la estética facial y el bienestar psicosocial del paciente. Su tratamiento exitoso, al final del crecimiento, exige un diagnóstico preciso y un abordaje coordinado entre ortodoncia y cirugía maxilofacial para lograr resultados estables y satisfactorios.
Objetivo: describir el enfoque diagnóstico-terapéutico y los resultados obtenidos tras el tratamiento ortodóncico-quirúrgico combinado en un paciente con prognatismo mandibular severo y mordida abierta anterior.
Presentación del caso: paciente masculino de 18 años, con antecedente familiar de prognatismo, acudió por compromiso estético y funcional. El examen clínico reveló aumento del tercio facial inferior, incompetencia labial, desviación mandibular derecha, relación molar clase iii bilateral, resalte invertido de -6 mm y mordida abierta anterior de 2.7 mm. El análisis cefalométrico confirmó el diagnóstico de discrepancia esquelética severa (anb= -6°). El tratamiento consistió en una fase ortodóncica prequirúrgica de descompensación, seguida de una cirugía bimaxilar y una fase ortodóncica final de detailing oclusal.
Conclusiones: El manejo ortodóncico-quirúrgico integrado corrigió eficazmente esta deformidad esquelética compleja. Se obtuvo una oclusión Clase I estable, se eliminó la mordida abierta y se mejoró significativamente la armonía facial. Este caso destaca la importancia crucial del trabajo en equipo multidisciplinario y de una planificación secuencial para abordar simultáneamente la función y la estética, impactando positivamente en la calidad de vida del paciente.
Palabras clave: Prognatismo mandibular; Mordida abierta; Cirugía ortognática; Ortodoncia; Clase III esquelética.
INTRODUCTION
Dentomaxillofacial disharmonies represent a group of complex structural alterations of multifactorial etiology—involving the interaction of genetic and environmental components—that manifest as dental malpositions and/or discrepancies in the development of the maxillary bones (1). These anomalies result in an inadequate skeletal and occlusal relationship between the maxilla and mandible, compromising not only facial aesthetics but also essential functions of the stomatognathic system, such as mastication, phonation, and swallowing (1,2).
Within this spectrum, the combination of mandibular prognathism and anterior open bite (AOB) constitutes one of the most complex diagnostic and therapeutic challenges in orthodontics and maxillofacial surgery (3). Mandibular prognathism, a diverse clinical phenotype, is characterized by a relative protrusion of the mandible in relation to the maxilla. This condition can be due to excessive mandibular growth, deficient maxillary development, or, more commonly, a combination of both factors (4). Frequently, this skeletal pattern is associated with an anterior open bite, in which vertical contact between the anterior dental segments is lost (5).
The prevalence of mandibular prognathism varies among populations, affecting approximately 1% to 3% of the world's population. Epidemiological studies indicate a prevalence of around 15% in Caucasian populations, 13% in Asian groups, and up to 27.4% in the Cuban population, which underscores its relevance as an oral health problem (6,7). The etiology of anterior open bite is also multifactorial, and can originate from skeletal imbalances (such as an increased vertical facial pattern or a prominent mandible), dentoalveolar compensations (tooth inclinations), or the persistence of deleterious functional habits, such as tongue thrust (8).
The therapeutic approach to these deformities should aim for long-term occlusal and skeletal stability, along with the restoration of satisfactory facial harmony. The range of options is broad and must be individualized, from compensatory orthodontic treatments (camouflage) in mild to moderate cases to surgical procedures that reposition the jaws through osteotomies. In severe deformities, bimaxillary orthognathic surgery is usually the preferred option to achieve a functional occlusal relationship, a balanced facial profile, and stable closure of the open bite (9,10).
In summary, there are three main treatment pathways: growth modification in developing patients, orthodontic camouflage, and orthognathic surgery (11). When the severity of the skeletal discrepancy indicates the need for a surgical approach, success depends critically on a comprehensive, multidisciplinary approach. This team, comprised of orthodontists, maxillofacial surgeons, and other specialists, is responsible for establishing an accurate diagnosis, predicting aesthetic and functional outcomes, and implementing a sequential treatment plan that addresses the patient's specific problems, with the ultimate goal of achieving lasting functional occlusion and facial harmony (12).
Therefore, considering the complexity of managing mandibular prognathism associated with an open bite, the authors of this study aim to describe the diagnostic and therapeutic approach and the results obtained after combined orthodontic and surgical treatment in a patient with severe mandibular prognathism and an anterior open bite.
CASE PRESENTATION
We present the case of an 18-year-old male patient who visited the Maxillofacial Surgery Service of the “Faustino Pérez” Clinical Surgical Teaching Hospital with the primary complaint: “I want to look better and be able to bite properly.” During the medical history interview, the patient reported a family history of mandibular prognathism in his paternal grandfather. No active deleterious oral habits or relevant history of trauma were identified.
Extraoral Clinical Examination: (Figure 1)
The patient presented with a leptoprosopic facial biotype and a convex profile. A significant increase in the lower third of the face was observed, with bilabial incompetence at rest. A marked mandibular deviation to the right was evident, accompanied by a pronounced nasolabial fold and an obtuse nasolabial angle. (Figure 1)
 Figure 1. Frontal
and lateral views of the patient at rest, prior to treatment. Increased lower
facial volume, lip incompetence, right mandibular deviation, and a convex
profile are observed.
Figure 1. Frontal
and lateral views of the patient at rest, prior to treatment. Increased lower
facial volume, lip incompetence, right mandibular deviation, and a convex
profile are observed.
Intraoral Clinical Examination:
In centric occlusion, a bilateral Class III molar relationship (mesioclusion of more than one unit) was observed, with edge-to-edge contact in the canine region. (Figure 2) A reverse overjet of -6 mm was present between the upper and lower central incisors (16/46), along with an anterior open bite of 2.7 mm, and an absence of vertical contact between the anterior segments (Figure 2B). Masticatory function was unilateral, primarily on the left side.
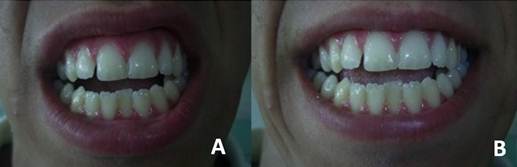
Figure 2. Preoperative intraoral examination. (A) Occlusal view of the upper and lower arches showing arch form and dental alignment. (B) Frontal view in occlusion showing severe anterior open bite and overjet.
Cephalometric Analysis:
The cephalometric values obtained confirmed the skeletal diagnosis:
1) Maxillobasal Relationship: SNA=79°, SNB=85°, ANB=-6° (indicative of a severe Class III skeletal discrepancy).
2) Vertical Pattern: Increased mandibular plane angle (FMA=43°), confirming a hyperdivergent facial pattern.
3) Dental Inclination: Compensatory proclination of the lower incisors (1NB=27°; 1-APog=5 mm) and retroclination of the upper incisors (1NA=20°).
4) Esthetic Analysis: The lips were significantly behind Ricketts' esthetic plane (upper lip: -3 mm; lower lip: +6 mm).
Study Model Analysis:
Revealed a positive skeletal-dental discrepancy in both arches, consistent with mild crowding and a slight transverse discrepancy (transverse micrognathism).
Multidisciplinary Treatment Plan:
Following a joint evaluation by the Orthodontics and Maxillofacial Surgery teams, a comprehensive plan was established, structured in three phases:
1) Pre-Surgical Orthodontic Phase: Aimed at dentoalveolar decompensation. The plan included arch alignment and leveling, correction of lower incisor proclination, and arch coordination, eliminating dental compensations to expose the true extent of the skeletal discrepancy and allow for optimal surgical repositioning.
2) Surgical Phase: Bimaxillary orthognathic surgery was planned with the following movements: maxillary impaction Le Fort I osteotomy (4 mm elevation), bilateral sagittal osteotomy of the mandibular rami for mandibular retraction (5 mm), and reduction and advancement mentoplasty (5 mm vertical reduction and 4 mm anterior projection) to harmonize the lower third of the face.
3) Post-Surgical Orthodontic Phase: Final occlusal detailing, closure of residual spaces, and establishment of a functional and stable occlusion, followed by retention.
Post-Treatment Result:
After completing the protocol, significant facial harmony was achieved, with reduction of the lower third of the face, improved lip competence, and correction of the mandibular deviation. Occlusally, a Class I molar and canine relationship was established, with positive functional overjet and overbite, and complete elimination of the open bite. (Figure 3)

Figure 3. Front and side views of the patient after treatment. Improvements to the facial profile, lip alignment, and harmony of the facial thirds are evident.
The treatment included psychological support for managing expectations and adapting to facial changes. The patient provided written informed consent for the publication of their images and clinical data.
DISCUSSION
This case illustrates the successful management of a complex dentofacial deformity using a coordinated orthodontic-surgical approach. The results obtained, consistent with the specialized literature, highlight the effectiveness of this protocol for simultaneously addressing the functional and aesthetic dimensions in patients with severe mandibular prognathism associated with anterior open bite (5).
The therapeutic decision in these cases should be based on a precise differential diagnosis, supported by clinical, model, and cephalometric analysis. It is essential to distinguish true mandibular prognathism from maxillary retrognathism or pseudo-Class III malocclusions, as the choice between orthodontic camouflage and surgery depends on this distinction. (10)
In the patient presented, the cephalometric values (ANB = -6°) and the severity of the skeletal discrepancy and open bite ruled out compensatory treatment. Camouflage has its limits and must be weighed against the expected facial profile and the patient's expectations. (16) In this case, the marked facial disharmony and the patient's reason for consultation made bimaxillary orthognathic surgery the ideal option to achieve comprehensive correction.
The surgical-orthodontic approach is structured in three interconnected phases. The presurgical phase, as performed here, has the critical objective of decompensation: eliminating compensatory dental inclinations (such as the proclination of the lower incisors) to expose the true skeletal discrepancy and allow for optimal maxillary repositioning during surgery (13). Subsequently, the bimaxillary surgical phase allows for correction of the discrepancy in all three planes of space. In accordance with the findings reported by Herrero Solano et al.,(9) the combination of an impaction Le Fort I osteotomy with mandibular retraction and mentoplasty not only normalized the occlusal relationship (ANB), but also dramatically improved the soft tissue profile and the esthetics of the lower third of the mouth, equally important objectives in contemporary surgery (13, 14).
Long-term stability and patient satisfaction are two key pillars for measuring success. Regarding stability, studies such as that by Fernández Pérez et al.,(12) indicate that, although minor skeletal relapses may occur in the first few months, the occlusion tends to remain stable thanks to dentoalveolar adaptation.
The patient presented here, during the follow-up period, has shown no signs of relapse, maintaining a functional Class I occlusion. Regarding satisfaction, we agree with other authors (15) that the psychosocial impact is profound. Correcting a visible facial deformity, such as the one our patient presented, transcends mere functionality, significantly improving self-esteem and quality of life—a subjective but crucial factor that validates multidisciplinary intervention.
Finally, it is imperative to mention the limitations and considerations of this approach. Orthognathic surgery carries inherent risks, such as the possibility of neurovascular complications, relapse, or alterations in sensation (13).
Furthermore, it requires a prolonged commitment from the patient and a high degree of coordination and communication between the orthodontist and surgeon. This case reinforces the notion that lasting success in managing complex dentomaxillofacial deformities lies in a comprehensive diagnosis, rigorous planning, and collaborative execution by the multidisciplinary team, always focused on the patient's specific needs and overall well-being. (5, 14)
CONCLUSIONS
The combined orthodontic and bimaxillary orthognathic surgery treatment proved effective in comprehensively correcting the Class III skeletal deformity with open bite in the patient presented. A functional Class I occlusion was achieved, along with the elimination of the open bite and a significant improvement in facial harmony, reducing the lower third of the face and correcting the mandibular deviation. This multidisciplinary approach not only restores masticatory function but also has a profound positive impact on the patient's self-esteem and quality of life, underscoring the importance of integrating aesthetic and functional objectives in the treatment plan.
BIBLIOGRAPHIC REFERENCES
1. Pérez BK, Vallejo ILA, Armas VAC. Tratamiento ortognático para corrección de clase III con ortodoncia pre y post quirúrgica. Caso clínico. Aula Virtual. [Internet] 2025 [cited 10/08/2025]; 5(12):e410. Available in: https://ve.scielo.org/scielo.php?script=sci_arttext&pid=S2665-03982024000202093
2. Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. 6th ed. St. Louis, MO: Elsevier; [Internet] 2019. Available in: https://shop.elsevier.com/books/contemporary-orthodontics/proffit/978-0-323-54387-3
3. Graber TM, Vanarsdall RL, Vig KW. Orthodontics: Current Principles and Techniques. 5th ed. Philadelphia: Elsevier; [Internet] 2016. Available in:https://shop.elsevier.com/books/orthodontics/graber/978-0-323-06641-9
4. Sánchez QD, García SL. Open bite: fisiología y manejo. In: López-Miranda J, editor. Manual de Ortodoncia. 3rd ed. Madrid: Editorial Médica; 2018. p. 345-65.
5. Guerrero WG, Valdivia IG. Ortodoncia y cirugía maxilofacial: un equipo multidisciplinario. Presentación de un caso clínico. Rev Mex Ortod. [Internet] 2014 [cited 10/08/2025]; 2(3):204-10. Available in: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=50699
6. Ruiz Feria N. Corrección de la morfología en un paciente con deformidad dento-maxilofacial severa. CCM [Internet]. 2025 [cited 10/08/2025];29:e5295. Available in: https://revcocmed.sld.cu/index.php/cocmed/article/view/5295
7. Morales Navarro D, Dago Farah S. Manejo integral estético de una anomalía dentofacial. Rev Cubana Estomatol. [Internet] 2020;57(1). [cited 10/08/2025]. Available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75072020000100018
8. Barrero Castillo TC, Viltres Pedraza GR, Arcia Cruz L, Collejo Rosabal Y, Estrada Viltres LC. Factores hipotéticamente influyentes en la aparición del micrognatismo transversal en escolares. Multimed. [Internet] 2021 [cited 10/08/2025];25(6):e1996. Available in: http://www.revmultimed.sld.cu/index.php/mtm/article/view/1996
9. Herrero Solano Y, Soto Cantero L, Ros Sanatana M, Arias Molina Y, Almeida Boza EX. Tratamiento de la clase III esquelética máxilo-madibular con twin block. Rev Haban Cienc Méd. [Internet] 2020 [cited 10/08/2025];19(2). Available in: http://www.revhabanera.sld.cu/index.php/rhab/article/view/3114
10. Dalaie K, Behnazz M, Banihashem S, Motamedian SR, Yassaee VR. Asociación de los polimorfismos P561T y C422F del gen receptor de la hormona del crecimiento con dimensiones faciales. J Oral Res. [Internet] 2019 [cited 10/08/2025];8(6). Available in: https://dialnet.unirioja.es/servlet/articulo?codigo=8059612
11. Tapia-Silgado M, Sánchez-Barroso Y, Urquijo-Berrocal L, Mondragón-Bohórquez S, Plazas-Roman J. Hábitos orales parafuncionales: asociación con maloclusiones en niños de 7 a 12 años asistentes a una clínica odontológica de Cartagena. Acta Bioclínica. [Internet] 2025 [cited 10/08/2025]; 15(31):175-94. Available in: http://erevistas.saber.ula.ve/index.php/actabioclinica/article/view/21541
12. Fernández Pérez E, Morán Gusieva I, Batista González NM, de Armas Gallegos LI. Disyunción maxilar con Hyrax en paciente síndrome Clase III y mordida abierta anterior. Habana 2018. Rev Latinoam Ortodoncia Odontopediatría. [Internet] 2018. [cited 10/08/2025]. Available in: https://www.ortodoncia.ws/publicaciones/2018/art-28/
13. Torres Rodríguez S, Polit Luna A. Cambios cefalométricos en pacientes con prognatismo y pseudo prognatismo mandibular pre y postquirúrgicos. Estudios Odontológicos de la Universidad de Guayaquil. [Internet] 2023 [cited 10/08/2025]; 6(1):56-65. Available in: https://revistas.ug.edu.ec/index.php/eoug/es/article/view/82/114
14. Ubilla Mazzini W, Apolo Morán J, Pazmiño Rodríguez E, Arroyo Apolo D. Maloclusión Clase III: Opciones de tratamiento para mejorar la estética y función del paciente. Rev Cient Univ Odontol Dominic. [Internet] 2024 [cited 10/08/2025]; 12(1). Available in: https://revistacientificauod.wordpress.com/wp-content/uploads/2024/06/revision-ubilla-apolo-pazmino-arroyo.pdf
15. Bioti Torres AM, Torres Lima M, Rezk Díaz A, Morejón Fernández AC. Maloclusión clase III tratada con máscara facial. Rev Cienc Méd. [Internet] 2018 [cited 10/08/2025];22(2):167-72. Available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-31942018000200020
16. García Menéndez M, Ruiz Gálvez OI, Abull Jauregui J, Hernández Gálvez Y, Ducasse Olivera PA. Tratamiento integral de la clase III esquelética severa, mordida abierta y asimetría facial. Rev Cubana Estomatol [Internet]. 2022 [cited 10/08/2025]; 59(4). Available in: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75072022000400002&lng=es
AUTHORSHIP STATEMENT
LMGG: Conceptualization, Data Curation, Formal Analysis, Research, Methodology, Resources, Supervision, Validation, Visualization, Writing, Writing - Review and Editing.
AMC: Conceptualization, Research, Resources, Visualization, Writing - Review and Editing.
MSV: Conceptualization, Research, Resources, Visualization, Writing - Review and Editing.
IPP: Conceptualization, Formal Analysis, Research, Methodology, Resources, Supervision, Visualization, Writing - Review and Editing.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING SOURCES
The authors received no funding for the development of this article.