CASE PRESENTATION
Advanced mandibular ameloblastoma: a case report
Ameloblastoma mandibular avanzado: a propósito de un caso
Pedro Alberto Pérez Pagés 1*, https://orcid.org/0000-0002-2103-407x
Maria Teresa Lima Reyna 1, https://orcid.org/0000-0002-7406-1186
Eric Gustavo Espino Hernández 2, https://orcid.org/0009-0005-4547-2452
Eliovanis Perera Cadavieco 2, https://orcid.org/0009-0004-9304-6100
1 Faustino Pérez Provincial Clinical-Surgical-Teaching Hospital. Matanzas, Cuba.
2 University of Medical Sciences of Matanzas. Faculty of Medical Sciences of Matanzas “Dr. Juan Guiteras Gener”. Matanzas, Cuba.
* Corresponding author: pedroalbertoperezpages@gmail.com
Received: 23/09/2025
Accepted: 22/02/2026
How to cite this article: Pérez-Pagés PA; Lima-Reyna MT; Espino-Hernández EG; Perera-Cadavieco E. Advanced mandibular ameloblastoma: a case report. MedEst. [Internet]. 2026 [cited access date]; 6:e485. Available in: https://revmedest.sld.cu/index.php/medest/article/view/485
ABSTRACT
Introduction: ameloblastoma is the most frequent benign epithelial odontogenic tumor, characterized by slow growth, high recurrence rate, and extensive bone destruction capacity. Delayed diagnosis results in large lesions with functional compromise and severe facial deformities.
Objective: to describe a case of advanced mandibular ameloblastoma in a geriatric patient, emphasizing the implications of delayed diagnosis in surgical management.
Case presentation: 78-year-old male patient with progressive volume increase in left hemiface and neck of 10 years evolution. Presented mechanical dysphagia, dysarthria, and recurrent oral bleeding. Physical examination revealed 10 cm diameter tumor, stony consistency, without inflammatory signs. Computed tomography showed multilocular osteolytic lesion of 7.2 × 9.9 cm occupying body and ascending ramus of left hemimandible, with destruction of more than 50% of bone. Incisional biopsy confirmed ameloblastoma. Radical hemimandibulectomy with disarticulation and safety margins was performed under general anesthesia. Definitive histopathological study confirmed follicular ameloblastoma. Postoperative evolution was satisfactory, without complications, discharged on tenth day.
Conclusions: delayed diagnosis of ameloblastoma in geriatric patients determines the need for extensive surgical resections with greater morbidity. This case underscores the importance of systematic oral examination in routine stomatological practice for early detection of odontogenic lesions.
Keywords: Ameloblastoma; Maxillofacial Surgery; Oral neoplasms
RESUMEN
Introducción: el ameloblastoma es el tumor odontogénico epitelial benigno más frecuente, caracterizado por crecimiento lento, alta recurrencia y capacidad de destrucción ósea extensa. Su diagnóstico tardío origina lesiones de gran tamaño con compromiso funcional y deformidades faciales severas.
Objetivo: describir un caso de ameloblastoma mandibular avanzado en paciente geriátrico, enfatizando las implicaciones del diagnóstico tardío en el manejo quirúrgico.
Presentación del caso: paciente masculino de 78 años con aumento de volumen progresivo en hemicara y cuello izquierdos de 10 años de evolución. Presentaba disfagia mecánica, disartria y sangrado oral recurrente. El examen físico reveló tumoración de 10 cm de diámetro, consistencia pétrea, sin signos inflamatorios. La tomografía computarizada mostró lesión osteolítica multiloculada de 7.2 × 9.9 cm que ocupaba cuerpo y rama ascendente de la hemimandíbula izquierda, con destrucción de más del 50% del hueso. La biopsia incisional confirmó ameloblastoma. Se realizó hemimandibulectomía radical con desarticulación y márgenes de seguridad bajo anestesia general. El estudio histopatológico definitivo confirmó ameloblastoma folicular. La evolución postoperatoria fue satisfactoria, sin complicaciones, con alta médica al décimo día.
Conclusiones: el diagnóstico tardío de ameloblastoma en pacientes geriátricos determina la necesidad de resecciones quirúrgicas extensas con mayor morbilidad. Este caso subraya la importancia del examen bucal sistemático en la práctica estomatológica rutinaria para detección precoz de lesiones odontogénicas.
Palabras Clave: Ameloblastoma; Cirugía Maxilofacial; Neoplasias orales
INTRODUCTION
Ameloblastoma is the most common benign epithelial odontogenic tumor, characterized by locally aggressive behavior, a high recurrence rate, and extensive bone destruction. (1) It represents approximately 1% of all oral tumors and 11 % of odontogenic tumors, with a mandibular predilection (80 % of cases), particularly in the posterior region. (2,3) Although it can occur at any age, the highest incidence is between the third and fifth decades of life, with no sex predilection. (4)
Clinically, it manifests as slow, painless growth, frequently asymptomatic in its initial stages, which contributes to late diagnoses with large lesions. (5) Radiographically, it appears as a well-defined, unilocular or multilocular radiolucent lesion, often associated with an impacted tooth. (2) The World Health Organization classification (ICD-11: 2F30.01) distinguishes solid/multicystic, uncystic, desmoplastic, and peripheral variants; The first three exhibit aggressive behavior with irregular bone infiltration that justifies radical surgical management. (1,6)
Treatment constitutes the main therapeutic challenge. Conservative approaches (enucleation, curettage) present recurrence rates of 55-90 %, while resection with safe bone margins (10-15 mm) reduces recurrence to 10-15 %. (7,8) This need for radical surgery is accentuated in late diagnoses, where prolonged growth causes massive destruction of the mandibular architecture, functional impairment (mastication, phonation), and severe facial deformities. (5,9)
Presentation in the eighth decade of life with a decade-long evolution and destruction of more than 50 % of the mandible is a clinical rarity that underscores the importance of early detection in routine dental practice.
The aim of this report is to describe a case of advanced mandibular ameloblastoma in a geriatric patient, emphasizing the implications of late diagnosis on surgical and functional management.
CASE PRESENTATION
We report the case of a 78-year-old Black male patient who came to the Maxillofacial Surgery Service of the “Faustino Pérez” Clinical-Surgical-Teaching Hospital in Matanzas, Cuba.
The patient had a history of smoking and chronic alcoholism. He reported a progressive and painless increase in volume on the left side of his face and cervical region, which had been present for approximately ten years, attributing its onset to a traumatic event (a fall). The patient's primary complaint was difficulty eating (mechanical dysphagia) and speaking (dysarthria), in addition to recurrent episodes of minor oral bleeding.
Physical Examination
Extraoral: Marked facial asymmetry was noted due to increased volume in the left hemimandibular and submandibular region (Figure 1 A and B). Palpation revealed a well-defined, stony-hard mass approximately 10 cm in its largest diameter, not attached to the skin, painless, and without signs of acute inflammation. No cervical lymphadenopathy was palpated.
Intraoral: Severe bony expansion was observed, extending from the midline to the left retromolar region, with complete obliteration of the vestibular sulcus. The overlying mucosa was erythematous, ulcerated in some areas, and showed signs of recent bleeding. The absence of teeth was noted in the posterior left sector and the presence of root remnants in the anterior sector.

Figure 1: Facial asymmetry (A: frontal view, B: lateral view) due to tumor on the left side of the face.
Complementary Studies and Diagnosis:
1. Incisional Biopsy: Under local anesthesia, a tissue sample was taken for histopathological study, the result of which was consistent with ameloblastoma.
2. Laboratory Studies: Preoperative tests showed a profile consistent with chronic anemia (Hemoglobin: 8.3 g/dL, Hematocrit: 25%). The remaining parameters (complete blood count, blood glucose, renal function) were within normal limits.
3. Imaging Study (Computed Tomography - CT): The facial CT scan revealed an osteolytic, expansive, and multiloculated lesion with well-defined margins, completely occupying the body and ascending ramus of the left hemimandible, with dimensions of 7.2 x 9.9 cm in the axial plane and 7.8 x 9.2 cm in the coronal plane (Figures 2A and 2B). No pathological lymphadenopathy or invasion of adjacent soft tissues was evident, but there was bone destruction exceeding 50% of the mandible.
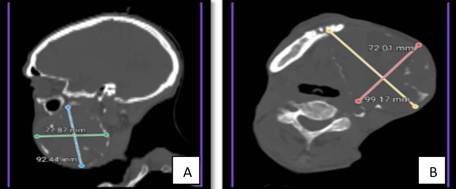
Figure 2: CT scans (A: sagittal, B: axial) showing the multiloculated osteolytic lesion in the left mandible.
Surgical Plan and Intervention:
Surgical intervention was decided upon under general anesthesia after tracheostomy. The surgical field was aseptically prepared with aqueous Hibatane for mucous membranes and 2% iodine tincture for the skin. A fenestrated drape and surgical field were applied. A vertical incision was made in the lower lip, continuing towards the left mandibular angle below the basilar border. Subsequent dissection of the lower cheek flap was performed. En bloc resection of the entire left hemimandible with disarticulation was performed; this procedure, known as hemimandibulectomy, was carried out to remove the tumor mass. Intraoral tissues were sutured with 4-0 polyglycolic acid, and extraoral tissues with metal staples (Figure 3 A and B). The late diagnosis in this patient led to the loss of more than 50% of the mandibular bone tissue.

Figure 3: Surgical procedure. (A) Hemimandibulectomy with disarticulation (B) Post-resection defect and repositioned flap.
Definitive Histopathological Study:
The surgical specimen was fully analyzed by the Department of Pathology. The
definitive histopathological diagnosis confirmed an ameloblastoma, follicular
subtype (Figure 4). The sections showed islands and cords of odontogenic
epithelium with palisading arrangement of peripheral cells, embedded in a
fibrous (desmoplastic) stroma, without evidence of cellular atypia or atypical
mitoses suggestive of malignant transformation.
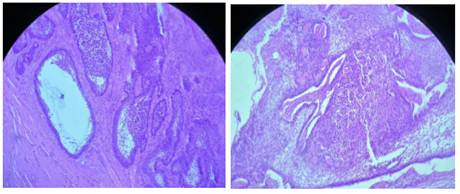
Figure 4: Photomicrographs (H/E, 100x and 200x) showing the follicular histological pattern of ameloblastoma.
Postoperative course:
The patient recovered satisfactorily without immediate complications. He was kept under observation in the postoperative care unit for 48 hours. Nasogastric tube feeding was initiated at 24 hours, and a soft diet was introduced on day 5. He was discharged on the tenth postoperative day. At one month of follow-up, the surgical wound showed good healing, with no signs of infection or tumor recurrence.
Informed consent: Written informed consent was obtained for the publication of her clinical case and associated images, guaranteeing the confidentiality of her personal data. The protocol was carried out following the ethical principles of the Declaration of Helsinki.
DISCUSSION
Ameloblastoma is an odontogenic neoplasm with complex biological behavior. In this case, the patient presented with the lesion at 78 years of age, which contrasts with the findings of Cardoso et al. (10), who place the main incidence between the third and fifth decades of life. However, the male predilection coincides with the slight prevalence reported by Ajilay V and Hegde S (11), with a ratio of 1.2:1.
A critical aspect in this case was the prolonged evolution of 10 years, which allowed the lesion to reach a size of approximately 10 cm. This slow and asymptomatic progression is characteristic of the entity, but in this patient, it resulted in extreme local aggressiveness. As Hashemi H et al. (12) point out, the infiltrative capacity of this tumor leads to extensive tissue destruction and facial deformity, elements that were evident in the marked mandibular asymmetry observed and that justified a radical surgical approach. (12)
Regarding location, the tumor was located in the mandible, consistent with the statistics of García Cruz et al., (14) who maintain that 80 % of these tumors appear in this bone, primarily affecting the ascending ramus. Although the etiology is debated, the relationship with impacted teeth is an important consideration in the analysis of the origin of this case, likely deriving from the enamel epithelium. (13)
Despite the size of the mass (10 cm), no signs of malignant transformation or metastasis were evident. This agrees with the findings of Delarue et al., (15) who state that metastasis is an extremely rare event (less than 1% of cases), even in large tumors. However, the magnitude of the lesion necessitated a hemimandibulectomy, an invasive treatment that reflects the consequences of late detection.
Finally, this clinical case clearly illustrates that, although ameloblastoma is benign, a delay in diagnosis—in this case, a decade—transforms the patient's functional prognosis. While early detection allows for minimally invasive interventions, this patient's prolonged progression resulted in serious sequelae such as massive bone loss and the need for complex reconstruction. This reaffirms that early diagnosis is the determining factor in preserving oral function, speech, and quality of life, mitigating the psychological impact of extensive resective surgeries.
CONCLUSIONS
This report presents a case of a large mandibular ameloblastoma with a ten-year history in an elderly patient. The late diagnosis necessitated a radical hemimandibulectomy, confirming that resection with wide margins remains the standard treatment in advanced stages of this locally aggressive neoplasm. This case underscores the critical importance of early detection through a high index of clinical suspicion in routine dental practice, as only early identification allows for conservative interventions that preserve oral function, facial aesthetics, and the patient's quality of life.
BIBLIOGRAPHIC REFERENCES
1. Hernández Gálvez Y, Ducasse Olivera PA, Abull Jauregui J. Ameloblastoma mandibular: resultados del tratamiento quirúrgico. AACC [Internet]. 2021 [cited 19/09/2025];11(1). Disponible en: https://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S230401062021000100022&lng=es&tlng=es
2. Rabelo CA. Ameloblastoma mandibular convencional en etapa avanzada. CCM [Internet]. 2022 [cited 19/09/2025];26(1):218-26. Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=113261
3. Soriano Cueto Y, Reyna Villasmil E. Ameloblastoma unquístico de mandíbula. RRMC [Internet]. 2023 [cited 19/09/2025];32(2). Disponible en: https://revistas.facusalud.edu.co/index.php/repertorio/article/view/1251/2459
4. Troya BE, Batista VM, Díaz DD. Hemimandibulectomía por ameloblastoma multiquístico. A propósito de un caso. RME [Internet]. 2021 [cited 19/09/2025];43(2). Disponible en: https://scielo.sld.cu/scielo.php?pid=S1684-18242021000203239&script=sci_abstract&tlng=en
5. Mendoza Álvarez S, Alonso Moctezuma A, Salgado Chavarría F. Ameloblastoma: historia y patogénesis molecular actual. RMCBM [Internet]. 2024 [cited 19/09/2025];20(1). Disponible en: https://www.medigraphic.com/pdfs/cirugiabucal/cb-2024/cb241f.pdf
6. Sánchez JG, Hernández FO, Hernández DY. Reemplazo mandibular con prótesis personalizada de titanio posterior a la exéresis de ameloblastoma. RCE [Internet]. 2021 [cited 19/09/2025];58(3). Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=109788
7. Suhani G. Ameloblastoma: una revisión narrativa actualizada de un tumor enigmático. Cureus [Internet]. 2022 [cited 19/09/2025];14(8):e27734. Disponible en: https://assets.cureus.com/uploads/review_article/pdf/108348/20220916-25113-8tjhft.pdf
8. Decani S, Quatrale M, Caria V, Moneghini L, Varoni EM. Peripheral Ameloblastoma: A Case Report and Review of Literature. JCM. 2024;13(22):6714. DOI:10.3390/jcm13226714
9. Hu K, Zhang X, Chen R, Li X. Recent methods for the diagnosis and differentiation of ameloblastoma: a narrative review. TF. 2024;17(1). DOI:10.1080/26895293.2024.2354675
10. Cardoso LB, Lopes IA, Ikuta CRS, Capelozza ALA. 2020. Study between panoramic radiography and cone beam-computed tomography in the diagnosis of ameloblastoma, odontogenic keratocyst, and dentigerous cyst. J Craniofac Surg. 31(6):1747–1752. doi:10.1097/SCS.0000000000006538.
11. Ajilay V, Hegde S. Ameloblastomas vs recurrent ameloblastomas: a systematic review. JOMOS [Internet]. 2022 [cited 20/09/2025];28(1). Disponible en: https://www.jomos.org/articles/mbcb/full_html/2022/01/mbcb210101/mbcb210101.html
12. Hashemi H, Näsman A, Farzad P. Peripheral ameloblastoma presenting as a solid mass in the temporal fossa: A case report and review of the literature. OMSC [Internet]. 2022 [cited 20/09/2025];8(4). Disponible en: https://www.sciencedirect.com/science/article/pii/S2214541922000438
13. Chai ZK, Mao L, Chen H, Sun T-G, Shen X-M, Liu J, Sun Z-J. 2021. Improved diagnostic accuracy of ameloblastoma and odontogenic keratocyst on cone-beam CT by artificial intelligence. Front Oncol. 11:793417. doi:10.3389/fonc.2021.793417.
14. García Cruz CA, Soler Izquierdo E, Niño Peña A, Batista Marrero K. Ameloblastoma unquístico plexiforme de maxilar superior. A propósito de un caso. CCM [Internet]. 2022 [cited 21/09/2025];26(4). Disponible en: https://revcocmed.sld.cu/index.php/cocmed/article/view/4513/2218
15. Delarue M, Derruau S, Troyon P, Bogard F, Polidori G, Mauprivez C. 2021. Medical infrared thermography in peri-operative management of peripheral ameloblastoma: A case report. Photodiagnosis Photodyn Ther. 34:102167. doi:10.1016/j.pdpdt.2020.102167.
AUTHORSHIP STATEMENT
PAPP: conceptualization, research, methodology, data curation, formal analysis, drafting of the original manuscript, drafting of the revision and editing.
MTLR: conceptualization, data curation, formal analysis.
EGEH: research, methodology, drafting of the original manuscript.
EPC: methodology, drafting of the original manuscript, drafting of the revision and editing.
FUNDING SOURCES
No external funding was received.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest.
USE OF ARTIFICIAL INTELLIGENCE
The authors declare that no artificial intelligence was used in the writing of this manuscript.