RESEARCH ARTICLE
Risk factors for breast cancer in women from a family medical practice
Factores de riesgo del cáncer de mama en mujeres de un consultorio médico de familia
Laudys Rosa Blanco Hernández 1, https://orcid.org/0000-0002-5357-5970
Olga González La Nuez 2, https://orcid.org/0000-0003-2519-1301
Ivette Valdés Gazmuri 3, https://orcid.org/0000-0002-0016-2785
Leysa Buides Secada 4, https://orcid.org/0000-0003-2831-2834
Luis Secada Cárdenas 5, https://orcid.org/0000-0002-1838-1767
1 “José Ramón López Tabrane” Provincial Ginecobstetric Teaching Hospital. Matanzas, Cuba.
2 University of Medical Sciences of Matanzas. Matanzas, Cuba.
3 “José Jacinto Milanés” Teaching Polyclinic. Matanzas, Cuba.
4 University of Havana. Havana, Cuba.
5 Provincial Government of Matanzas. Matanzas, Cuba.
* Corresponding author: rosalaudys@gmail.com
Received: 04/01/2026
Accepted: 30/03/2026
Published: 13/04/2026
How to cite this article: Blanco-Hernández LR, González-La-Nuez O, Valdés-Gazmuri I, Buides-Secada L, Secada-Cárdenas L. Risk factors for breast cancer in women from a family medical practice. MedEst. [Internet]. 2026 [cited access date]; 6:e497. Available at: https://revmedest.sld.cu/index.php/medest/article/view/497
ABSTRACT
Introduction: Breast cancer is the leading cause of cancer death among women worldwide and the second in Cuba. Identifying risk factors in primary care is essential for implementing preventive strategies.
Objective: To identify breast cancer risk factors in the female population of Family Medical Office No. 24 at "José Jacinto Milanés" Polyclinic, Matanzas, Cuba.
Methods: An observational, descriptive, cross-sectional study was conducted from February to December 2025. A total of 421 women aged 15-90 years were included through convenience sampling. A validated structured questionnaire was applied. Sociodemographic variables, clinical risk factors, and breast self-examination practices were analyzed. Statistical processing was performed using SPSS v22, with 95 % confidence level.
Results: Mean age was 47.94±20.70 years; 46.56 % were ≥60 years old. The most prevalent risk factors were early menarche (50.83 %), arterial hypertension (45.13 %), late menopause (42.99 %), first childbirth after 30 years (33.49 %), and nulliparity (23.75 %). Only 9.03 % performed breast self-examination, and 23.75% knew the appropriate timing for its practice.
Conclusions: The most prevalent risk factors were early menarche, arterial hypertension, late menopause, first childbirth after 30 years, and nulliparity. The low frequency of breast self-examination identifies a critical gap in secondary prevention requiring educational interventions in primary care.
Keywords: Risk Factors, Breast Cancer, Breast Self-Examination, Prevention, Primary Health Care.
RESUMEN
Introducción: El cáncer de mama constituye la primera causa de muerte por cáncer en mujeres a nivel mundial y la segunda en Cuba. La identificación de factores de riesgo en atención primaria resulta fundamental para la implementación de estrategias preventivas.
Objetivo: Identificar los factores de riesgo de cáncer de mama en la población femenina del Consultorio Médico de la Familia No. 24 del Policlínico "José Jacinto Milanés", Matanzas, Cuba.
Métodos: Estudio observacional, descriptivo, de corte transversal, realizado entre febrero y diciembre de 2025. Se incluyeron 421 mujeres de 15-90 años mediante muestreo por conveniencia. Se aplicó cuestionario estructurado validado. Se analizaron variables sociodemográficas, factores de riesgo clínicos y prácticas de autoexamen. El procesamiento estadístico se realizó con SPSS v22, con nivel de confianza del 95 %.
Resultados: La edad media fue 47,94±20,70 años; el 46,56 % tenía ≥60 años. Los factores de riesgo más prevalentes fueron menarquia precoz (50,83 %), hipertensión arterial (45,13 %), menopausia tardía (42,99 %), primer parto posterior a los 30 años (33,49 %) y nuliparidad (23,75 %). Solo el 9,03 % realizaba autoexamen de mama y el 23,75 % conocía el momento adecuado para su práctica.
Conclusiones: Los factores de riesgo más prevalentes fueron menarquia precoz, hipertensión arterial, menopausia tardía, primer parto posterior a los 30 años y nuliparidad. La baja frecuencia de autoexamen de mama identifica una brecha crítica en la prevención secundaria que requiere intervenciones educativas en atención primaria.
Palabras clave: Factores de Riesgo, Cáncer de Mama, Autoexamen de Mama, Prevención, Atención Primaria.
INTRODUCTION
Breast cancer constitutes the accelerated, disordered, and uncontrolled proliferation of epithelial cells with genetic alterations that favor the continuity of the cell cycle, originating in the different tissues of the mammary gland. (1) Its neoplastic cells can spread through lymphatic or hematogenous invasion, leading to metastasis in distant organs. (2) Although it can occur in both sexes, more than 99 % of cases occur in women. (2)
This neoplasm has a multifactorial origin and constitutes a heterogeneous entity with distinct histological and molecular subtypes, each with specific epidemiological, prognostic, and therapeutic patterns. (3,4) Early diagnosis represents the primary strategy to reduce mortality from this disease, (4) with knowledge of risk factors being a fundamental element for the identification of vulnerable populations. (4,5)
The World Health Organization defines a risk factor as any trait, characteristic, or exposure that increases the likelihood of developing a particular disease. (4) In breast cancer, these factors are classified into non-modifiable and modifiable. Among the former, advanced age, a first-degree family history of breast cancer, hereditary genetic mutations (BRCA1 and BRCA2), early menarche, and late menopause are prominent. (4,5) Modifiable factors include nulliparity, the absence or short duration of breastfeeding, postmenopausal overweight and obesity, physical inactivity, alcohol consumption, and smoking. (4)
The global distribution of breast cancer reflects a complex interaction between genetic, environmental, and socioeconomic determinants. (5) In 2022, this neoplasm ranked as the one with the highest incidence among women worldwide and as the leading cause of cancer death in females, with 666,000 deaths. (5,6) The Americas accounted for nearly a quarter of the new global cases, with more than 525,000 diagnoses. (7) Notably, in Latin America and the Caribbean, 31 % of cases and 21 % of deaths occurred in women under 50 years of age, figures significantly higher than those recorded in North America. (7)
In Cuba, breast cancer constitutes the second leading cause of cancer mortality in females. The 2024 Health Statistical Yearbook reported a mortality rate of 35.8 per 100,000 women and a premature mortality rate (30-69 years) of 31.1 per 100,000, higher than that of the preceding year. (8) The province of Matanzas presents a particularly high incidence within the national context, with 1,795 women deceased from this cause in 2024, (8) highlighting the need for research that characterizes the risk factors in this region.
Faced with this issue, Cuba's National Public Health System established the National Program for the Early Diagnosis of Breast Cancer, whose fundamental objectives include minimizing morbidity, improving survival, and optimizing quality of life through less mutilating treatments. (6,9) The identification of risk factors in the population managed in primary health care is essential for the implementation of primary prevention strategies and the direction of resources toward the most vulnerable groups.
Previous studies conducted in Cuba and in the province of Matanzas have identified various risk factors in different population groups, (1,9-12) agreeing that the knowledge of these elements by women and health personnel constitutes a fundamental tool for early diagnosis and the modification of risky behaviors. However, gaps persist in the systematic application of breast self-examination and in the acquisition of knowledge regarding risk factors by health service users.
The authors identified as a public health problem that the incidence of breast cancer at early ages shows an increasing trend, (2) which demands community interventions oriented toward the modification of avoidable risk factors. They consider that if women know and recognize these factors, they will be in a better position to detect early signs and symptoms and seek consultation in a timely manner.
The objective of the present study was to identify the risk factors for breast cancer in the female population belonging to Family Doctor's Office No. 24 of the "José Jacinto Milanés" Teaching Polyclinic, in the municipality of Matanzas, during the period of February-December 2025.
METHODS
Study design
An observational, descriptive, cross-sectional study was conducted in the female population belonging to Family Doctor's Office No. 24 of the "José Jacinto Milanés" Teaching Polyclinic, in the municipality of Matanzas, Matanzas province, Cuba, during the period from February to December 2025.
Universe and sample
The universe was composed of all female patients (n=601) registered in the health area of Family Doctor's Office No. 24 at the end of January 2025. The sample was calculated using non-probabilistic convenience sampling, selecting 421 women who met the established eligibility criteria. The sample size was determined considering an estimated prevalence of risk factors of 50 %, a confidence level of 95 % (z=1.96), and a margin of error of 5 %, using the formula for finite populations: n=e2⋅(N−1)+Z2⋅p⋅qN⋅Z2⋅p⋅q
Where: N=601, Z=1.96, p=0.50, q=0.50, e=0.05. The calculation yielded a minimum sample size of 234 subjects; this was increased by 80 % to compensate for potential losses during data collection, resulting in n=421.
Eligibility Criteria
Inclusion criteria:
· Female patients aged ≥15 years.
· Patients who provided their written informed consent to participate in the research
Exclusion criteria:
· Patients who did not consent to participate in the study
· Patients absent from their home during three consecutive scheduled visits for data collection, conducted on alternating days and times
Elimination criteria:
· Patients who passed away during the study execution period, regardless of the cause of death
Study variables
The following variables were analyzed:
Sociodemographic variables:
· Age (attained years, categorized into ten-year groups)
· Skin color (white, mixed-race, black), self-reported
· Educational level (primary, lower secondary, mid-level technician, upper secondary/pre-university, university)
Clinical and risk factor variables:
· Age at first birth ≥30 years (yes/no)
· Nulliparity (yes/no)
· First-line family history: breast, ovarian, endometrial, or colon cancer in mother, sister, or daughter (yes/no)
· Second-line family history: breast cancer in grandmothers, aunts, or cousins (yes/no)
· Personal history of ovarian cancer, atypical hyperplasia, or previous breast cancer (yes/no)
· Early menarche: age of menarche onset <10 years (yes/no)
· Late menopause: age of menopause >55 years (yes/no), in postmenopausal women
· Postmenopausal obesity: body mass index ≥30 kg/m² (yes/no), in postmenopausal women
· Absence of breastfeeding or breastfeeding <3 months (yes/no).
· Sedentary lifestyle (yes/no)
· Smoking current or past (yes/no)
· Alcoholism (yes/no)
· Diabetes mellitus (yes/no)
· Arterial hypertension (yes/no)
Preventive practice variables
· Performance of breast self-examination (yes/no)
· Knowledge of the appropriate time to perform breast self-examination (yes/no)
Data collection instrument
A structured, self-administered questionnaire was developed with researcher assistance, adapted from the methodological criteria presented by Rigol Ricardo and Santiesteban Alba. (13) The instrument was validated through expert judgment (three gynecologists, two epidemiologists, and one methodologist) who evaluated content validity (Aiken's V ≥ 0.85 for all items) and clarity of wording. A pilot test was conducted with 20 women from Clinic No. 23 (not included in the final sample), yielding a Cronbach's alpha coefficient of 0.82 for global internal consistency.
Data collection procedure
The primary authors (LRBH and IVG) collected the information through direct interviews at the participants' homes, following a telephone appointment or coordination through the family doctor. Privacy was guaranteed during the interview, and the questionnaire was administered under conditions of confidentiality. Collection took place during the period of March–December 2025.
Statistical processing
The information was processed using the SPSS statistical package version 22.0 for Windows (IBM Corp., Armonk, NY, USA). Logical consistency analysis and database cleaning were performed. Qualitative variables were summarized using absolute frequencies (Fa) and relative frequencies (Fr, %). Quantitative variables were described using the arithmetic mean (x̄) and standard deviation (SD), after verifying normality through the Kolmogorov-Smirnov test. Fisher's skewness coefficient was calculated for the age variable. The level of statistical significance was established at p < 0.05.
Ethical aspects
The study was approved by the Institutional Ethics Committee of the University of Medical Sciences of Matanzas (Opinion No. 3/2025). Written informed consent was obtained from all participants after explaining the objectives, procedures, benefits, minimal risks, confidentiality, and the voluntary nature of participation. The information was anonymized through numerical coding, guaranteeing confidentiality and using it exclusively for scientific purposes. The study was conducted in accordance with the Ethical Principles for Medical Research Involving Human Subjects of the World Medical Association, Declaration of Helsinki, adopted at the 75th General Assembly, Helsinki, Finland, October 2024. (14)
RESULTS
The study included 421 women with ages ranging from 15 to 90 years. The mean age was 47.94 ± 20.70 years (median: 48 years; interquartile range: 28-68 years). Fisher's skewness coefficient was -0.093, indicating an approximately symmetrical distribution with a slight concentration of values below the mean. A higher relative frequency was observed in the age groups of 60 years or older (46.56 %), with a similar distribution between the 60-69 age group (23.04 %) and those 70 years or older (23.52 %).
Table 1. Distribution of patients according to age groups
|
Age (years) |
Fa |
Fr (%) |
|
<30 |
78 |
18,53 |
|
30-39 |
45 |
10,69 |
|
40-49 |
64 |
15,20 |
|
50-59 |
38 |
9,03 |
|
60-69 |
97 |
23,04 |
|
≥70 |
99 |
23,52 |
|
Total |
421 |
100,00 |
Source: Applied questionnaire. Fa: absolute frequency; Fr: relative frequency
Regarding self-reported skin color, patients with white skin predominated (246; 58.43 %), followed by mixed-race (108; 25.65 %) and black (67; 15.91 %) (Figure 1).
![]()
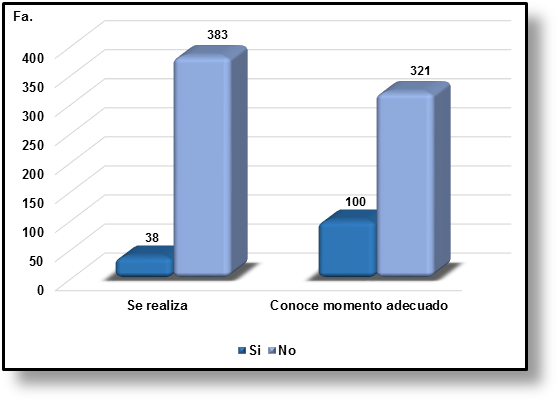
Figure 1. Distribution according to
skin color
Source: Applied questionnaire.
The most frequent educational level was upper secondary/pre-university (26.37 %), followed by university (22.80 %) and mid-level technician (21.85 %). A total of 28.98 % of the participants (n=122) had reached an upper secondary level or lower (Table 2).
Table 2. Distribution of patients according to educational level
|
Educational level |
Fa |
Fr (%) |
|
Primary |
49 |
11,64 |
|
Lower secondary |
73 |
17,34 |
|
Mid-level technician |
92 |
21,85 |
|
Pre-university |
111 |
26,37 |
|
University |
96 |
22,80 |
|
Total |
421 |
100,00 |
The most prevalent risk factors were early menarche (50.83 %), late menopause (42.99 %), arterial hypertension (45.13 %), first birth after age 30 (33.49 %), and nulliparity (23.75 %). Of the 100 nulliparous patients, 46 (46.0 %) were under 25 years of age, constituting a subgroup in which nulliparity corresponds predominantly to an early, incomplete reproductive age rather than a risk factor per se. Twenty-four patients (5.70 %) were identified with a first-line family history of breast, ovarian, endometrial, or colon cancer. Four patients (0.95 %) reported a personal history of previous breast cancer, and 32 patients (7.60 %) had a personal history of other related pathologies (ovarian cancer, atypical hyperplasia) (Table 3).
Table 3. Distribution of breast cancer risk factors in the studied sample
|
Risk factors |
Fa |
Fr (%) |
|
Hormonal and reproductive factors |
||
|
Early menarche (<10 years) |
214 |
50,83 |
|
Late menopause (>55 years) |
181 |
42,99 |
|
First birth >30 years |
141 |
33,49 |
|
Nulliparity |
100 |
23,75 |
|
Absence of breastfeeding or <3 months |
72 |
17,10 |
|
Anthropometric factors |
||
|
Postmenopausal obesity (BMI ≥30 kg/m²) |
67 |
15,91 |
|
Family history |
||
|
First-line family history* |
24 |
5,70 |
|
Second-line family history of breast cancer |
2 |
0,48 |
|
Personal history |
||
|
Arterial hypertension |
190 |
45,13 |
|
Diabetes mellitus |
45 |
10,69 |
|
History of ovarian cancer |
20 |
4,75 |
|
Atypical mammary hyperplasia |
12 |
2,85 |
|
Previous breast cancer |
4 |
0,95 |
|
Lifestyle |
||
|
Sedentary lifestyle |
57 |
13,54 |
|
Smoking |
56 |
13,30 |
|
Alcoholism |
6 |
1,43 |
Source: Applied questionnaire. *Breast, ovarian, endometrial, or colon cancer in mother, sister, or daughter. BMI: body mass index; Fa: absolute frequency; Fr: relative frequency
Regarding early detection practices, 38 patients (9.03 %) reported performing breast self-examination, while 383 (90.97 %) did not (Figure 2). Of the total sample, only 100 patients (23.75 %) knew the appropriate time to perform it (five days after the start of menstruation, or on a fixed date for menopausal women).
![]()
![]()
![]()

Figure
2. Breast
self-examination.
Source: Applied questionnaire.
DISCUSSION
The results of the present study show an epidemiological profile characterized by a mean age of 47.94±20.70 years and a significant concentration of patients in age groups of 60 years or older (46.56 %). These findings are consistent with international literature indicating that population aging is a fundamental determinant of the breast cancer burden. (2,15) The Spanish Society of Medical Oncology has reported an increase in incidence at early ages, (2) a phenomenon not predominately observed in our sample, where the highest frequency corresponds to advanced age groups. Mieles Resabala et al., (15) in a prevalence study conducted in Ecuador, documented that breast carcinomas are more frequent in older women, with approximately two out of every three invasive cancers detected in women aged 55 or older. This age distribution coincides with our results and reinforces the importance of screening programs oriented toward the postmenopausal population.
Age constitutes the most important non-modifiable risk factor; the short-term risk for a 70-year-old woman is nearly 10 times higher than that of a 30-year-old woman. (16) In our sample, 46.56 % of the participants were 60 years of age or older, which configures a population with increased susceptibility from an epidemiological perspective. However, it is relevant to note that 18.53 % of the sample corresponded to women under 30 years of age, a group in which primary prevention acquires particular relevance.
Regarding social determinants of health, 28.98 % of the participants had an educational level of lower secondary or lower. Ruiz et al. (19) have demonstrated that a low educational level is associated with limitations in the comprehension of health information and the adoption of preventive practices, a finding that gains relevance in our context given the low percentage of breast self-examination identified (9.03 %). The distribution by skin color showed a predominance of white (58.43 %), followed by mixed-race (25.65 %), and black (15.91 %). Although international literature reports higher breast cancer mortality in black women (41 % higher compared to white women), (18) our sample does not allow for establishing comparisons of mortality or incidence given its descriptive cross-sectional design.
Hormonal and reproductive risk factors were the most prevalent elements in our population. Early menarche (<10 years) affected 50.83 % of the participants, and late menopause (>55 years) affected 42.99 %. These findings coincide with previous studies conducted in Cuba. Hierrezuelo Rojas et al., (12) in a case-control study in the Playa municipality, Havana, identified statistically significant associations between early menarche (OR=5.65; p=0.001) and late menopause (OR=5.16; p=0.002) with breast cancer risk. The National Breast Cancer Coalition, the American Cancer Society, and the Centers for Disease Control and Prevention agree that prolonged exposure to endogenous estrogens, determined by the menarche-menopause interval, constitutes a well-established risk factor. (20,21)
First birth after age 30 was identified in 33.49 % of patients, and nulliparity in 23.75 %. However, of the 100 nulliparous patients, 46 % were under 25 years of age, suggesting that in this subgroup, nulliparity corresponds predominantly to ongoing reproductive age rather than a risk factor per se. Nulliparity and late first birth are associated with greater exposure to complete ovulatory cycles and, consequently, to endogenous estrogens. (16) González Santos, (7) in a characterization of patients in Holguín, Cuba, identified that between 11 % and 44.91 % of women had not breastfed or had done so for periods of less than six months, a figure comparable to our finding of 17.10 % for absence of breastfeeding or short duration (<3 months). Breastfeeding is inversely associated with breast cancer risk through mechanisms including the reduction of estrogen exposure and mammary epithelial differentiation. (16)
Arterial hypertension was the most prevalent risk factor (45.13 %), surpassing even the classic hormonal factors. Although hypertension is not traditionally considered a direct risk factor for breast cancer, recent studies suggest associations between cardiovascular diseases, metabolic syndrome, and oncological risk. (22) Postmenopausal obesity, present in 15.91 % of our sample, does constitute a well-established modifiable risk factor. Gálvez Vila et al. (23) point out that obesity is related to an increased risk in postmenopausal women not exposed to hormone therapy, and Hierrezuelo et al. (12) reported a significant association with OR=7.21. These findings underscore the importance of body weight control as a primary prevention strategy.
Sedentary lifestyle (13.54 %) and smoking (13.30 %) showed similar prevalence, while alcoholism was infrequent (1.43 %). Tobacco consumption, including passive exposure during childhood, has been associated with breast carcinoma through the presence of 20 mammary carcinogens identified in smoke. (24) Gram et al., (25) in the Norwegian Women and Cancer study, documented an 11 % increase in breast cancer risk among non-smoking women passively exposed during childhood. Alcohol consumption, although prevalent in our sample, constitutes a dose-dependent risk factor with no established safe threshold, acting through hormonal and non-hormonal pathways (DNA damage by acetaldehyde). (24)
First-line family history of breast, ovarian, endometrial, or colon cancer was identified in 5.70 % of the participants, and a personal history of breast cancer in 0.95 %. Rondón and Morales, (13) in a characterization in Guisa, Granma, Cuba, reported a family history in 39.1 % of patients with confirmed breast cancer—a figure higher than ours, which is expected given that their study included diagnosed cases. It is relevant to note that between 5 % and 10 % of breast cancers are hereditary, (16) and the absence of a family history does not exclude the risk of developing the disease.
The most concerning finding from a public health perspective was the low frequency of breast self-examination practice (9.03 %), with only 23.75 % of participants knowing the appropriate time for its performance. These results are lower than those reported by Lucas and Marín in Peru (58.6 % did not practice it, equivalent to 41.4 % who did), (28) and by Vargas et al. (29) in Cuba (46.1 % never performed it, equivalent to 53.9 % who had done so at some point). Martínez et al. (30) in Nicaragua identified that 69.4 % of women did not perform the self-exam correctly, suggesting that even when practiced, the technique may be inadequate.
This gap in secondary prevention becomes more significant considering that breast self-examination, although not proven to reduce mortality in randomized clinical trials, does contribute to early diagnosis and the empowerment of women regarding their health. (26,27) González Santos (7) emphasizes the need to intensify health education so that women take an active role in self-care. Authors point out that a high number of women attending breast pathology consultations detected their nodules through self-examination, (27) which validates its clinical utility despite its lack of epidemiological weight in mortality reduction.
The present study has the strength of having included more than 70 % of the eligible population universe, with a sample size adequate for descriptive estimates. However, the following methodological limitations should be noted.
In first place, the descriptive cross-sectional design does not allow for establishing causal relationships or calculating measures of association (relative risk, odds ratio); the identified factors are prevalent in the studied population but are not necessarily associated with a higher risk of developing breast cancer without comparison to a control group.
In second place, the non-probabilistic convenience sampling limits the generalization of the results to other populations; the sample may not be representative of the entire universe of women in the family doctor's office.
In third place, information on risk factors was obtained through self-reporting, with potential recall bias or social desirability bias, particularly for variables such as smoking, alcoholism, and self-examination practices. Finally, the measurement of some factors (early menarche, late menopause) may be affected by inaccuracy in remembering events that occurred decades ago.
The results of this study underscore the need to develop and implement robust educational interventions at the primary health care level, aimed at: (a) the modification of avoidable risk factors (obesity, sedentary lifestyle, smoking); (b) strengthening knowledge of non-modifiable risk factors for the early identification of symptoms; and (c) the systematic promotion of breast self-examination as a self-care practice, regardless of its controversy in international literature. The concentration of hormonal and reproductive factors in the population studied suggests that primary prevention strategies should begin at an early age, including education on menarche, family planning, and breastfeeding.
CONCLUSIONS
The most prevalent risk factors were early menarche (50.83 %), arterial hypertension (45.13 %), late menopause (42.99 %), first birth after age 30 (33.49 %), and nulliparity (23.75 %). The coexistence of multiple hormonal factors configures a susceptibility profile that requires differentiated preventive interventions. The low frequency of breast self-examination (9.03 %) and the limited knowledge regarding its appropriate timing (23.75 %) identify a critical gap in secondary prevention. The concentration of patients in groups aged 60 or older (46.56 %), combined with a high prevalence of non-modifiable factors and insufficient self-care, underscores the need to strengthen screening and health education programs in primary care.
BIBLIOGRAPHIC REFERENCES
1. Vasallo López C, Figueredo Garlobo LdlC, Blanco Paredes GdlC, López Ramírez N. Evaluation of the level of knowledge about breast cancer in women of childbearing age. EsTuSalud [Internet]. 2021 [cited 06/01/2026];3(3):e124. Available from: http://www.revestusalud.sld.cu/index.php/estusalud/article/view/124
2. Echavarría I. Breast cancer. Spanish Society of Medical Oncology [Internet]. 2025 [cited 06/01/2026]. Available from: https://seom.org/info-sobre-el-cancer/cancer-de-mama
3. Wu J, Fan D, Shao Z, Xu B, Ren G, et al. CACA Guidelines for holistic integrative management of breast cancer. Holist Integr Oncol [Internet]. 2022 [cited 06/01/2026];1(1):77. Available from: https://doi.org/10.1007/s44178-022-00007-8
4. Xiong X, Zheng LW, Ding Y, Chen YF, Cai YW, Wang LP, et al. Breast cancer: pathogenesis and treatments. Signal Transduct Target Ther [Internet]. 2025 [cited 06/01/2026];10:49. Available from: https://doi.org/10.1038/s41392-024-02108-4
5. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [Internet]. 2024 May-Jun [cited 06/01/2026];74(3):229-263. Available from: https://doi.org/10.3322/caac.21834
6. Cuba. Ministry of Public Health. National Breast Cancer Program. Havana: Editorial Ciencias Médicas; 2024.
7. González Santos L. Characterization of patients with breast cancer risk factors. Mayarí Polyclinic [thesis]. Holguín: University of Medical Sciences of Holguín; 2024 [cited 07/01/2026]. Available from: https://tesis.hlg.sld.cu/index.php?P=FullRecord&ID=3818
8. Escudero García A, Pérez Segura P. Breast cancer. Medicine - Accredited Continuing Medical Education Program [Internet]. 2025 [cited 07/01/2026];14(24):1412-1422. Available from: https://www.medicineonline.es/es-volumen-14-numero-24-sumario-S0304541225X00020
9. Pan American Health Organization. Breast cancer [Internet]. Washington: PAHO/WHO; 2025 [cited 07/01/2026]. Available from: https://www.paho.org/es/temas/cancer-mama
10. Ministry of Public Health of Cuba. Directorate of Medical Records and Health Statistics. Health Statistical Yearbook 2024. 53rd ed. Havana: MINSAP; 2025 [cited 07/01/2026]. Available from: http://bvscuba.sld.cu/anuario-estadistico-de-cuba/
11. Olivares-Alonso A, Placeres-Hernández JF, Rosales-Alcántara Y, Ramos-Reymont D, Delgado-Hernández I. Breast cancer risk factors in medical students from Matanzas. MedEst [Internet]. 2021 [cited 07/01/2026];1(2):e40. Available from: https://revmedest.sld.cu/index.php/medest/article/view/40
12. Hierrezuelo Rojas N, Cordoví Hierrezuelo M, Neira Hierrezuelo N. Risk factors associated with breast cancer in women of a health area. Revista Finlay [Internet]. 2023 [cited 07/01/2026];13(4):414-424. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S222124342023000400414
13. Rondón Carrasco J, Morales Vázquez CL. Clinical-epidemiological characterization of women with breast cancer in Guisa. Revista Médica Sinergia [Internet]. 2023 Aug [cited 07/01/2026];8(8):e1082. Available from: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=112529
14. Rigol Ricardo O, Santiesteban Alba S. Obstetrics and Gynecology. 3rd ed. Havana: ECIMED; 2014.
15. Mieles Resabala RM, Valeria Pico M, Marín Pérez A, Cedillo Balcáza J. Prevalence study of breast cancer risk factors in a Specialty Hospital in Manabí – Ecuador. Oncology (Ecuador) [Internet]. 2024 [cited 07/01/2026];34(3):131-141. Available from: https://doi.org/10.33821/764
16. Obregón Sánchez NH, Moreno González MM, Guzmán Ortiz E, Trujillo Hernández PE, Lara Reyes BJ. Risk factors for breast cancer in women with a family history. Integrative review. Salud Uninorte [Internet]. 2024 [cited 08/01/2026];40(1):273-294. Available from: https://dx.doi.org/10.14482/sun.40.01.741.258
17. Estrada Rodríguez Y, Oviedo Pérez K, Naranjo Lima S, Boris Miclin CD, Hoyos Mesa AJ, Almeida Rodríguez Ángel F. Characterization of adolescent pregnant women at the Samuel Fernández Polyclinic in the municipality of Matanzas in 2020. scalpelo [Internet]. 2025 [cited 08/01/2026];5. Available from: https://rescalpelo.sld.cu/index.php/scalpelo/article/view/223
18. Giaquinto AN, Sung H, Newman LA, Freedman RA, Smith RA, Star J, et al. Breast cancer statistics 2024. CA Cancer J Clin [Internet]. 2024 [cited 08/01/2026];74(6):477-495. Available from: https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21863
19. Ruíz M, Aginagalde A, Llano J. Social determinants of health in Spain (2010-2021). Rev Esp Salud Pública [Internet]. 2022 May [cited 08/01/2026];96:e202205041. Available from: https://dialnet.unirioja.es/servlet/articulo?codigo=8620643
20. National Breast Cancer Coalition. Breast cancer facts and figures [Internet]. Washington: NBCC; 2025 [cited 08/01/2026]. Available from: https://www.stopbreastcancer.org
21. American Cancer Society. Cancer Facts & Figures 2023 [Internet]. Atlanta: ACS; 2023 [cited 08/01/2026]. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2023/2023-cancer-facts-and-figures.pdf
22. Boris Miclin Miclin CD, Estrada Rodríguez Y, Álvarez Pérez RJ, Corría Milán II. Arterial hypertension and pregnancy: an updated review of the subject [Internet]. In: Proceedings of CARDIOÁVILA 2024. 2024 [cited 08/01/2026]. Available from: https://cardiologiaca.sld.cu/index.php/cardiocav/2024/paper/viewPaper/10
23. Gálvez Vila RM, Naranjo Lima S, Gallego Sánchez JA, Román Rodríguez A, Estrada Rodríguez Y. Prevalence of obesity in women of childbearing age at medical office #12. Colón, Matanzas, 2024 [Internet]. In: APSGibara2025. 2025 [cited 08/01/2026]. Available from: https://apsgibara2023.sld.cu/index.php/APSGibara2025/2025/paper/viewFile/608/968
24. Adrover Cebrián E, Alfaro Galán L, Algara López M, Alonso Osorio MJ, Álvarez Vinuesa M, Barreiro Mont S, et al. Lifestyle and breast cancer: actions before, during and after treatment. 2nd ed. Madrid: Spanish Society of Senology and Breast Pathology; 2023 [cited 08/01/2026]. Available from: https://sespm.es/wp-content/uploads/2023/03/Libro-MONOGRAFIA-SESPM-2022web.pdf
25. Gram IT, Wiik AB, Lund E, et al. Never-smokers and the fraction of breast cancer attributable to second-hand smoke from parents during childhood: the Norwegian Women and Cancer Study 1991-2018. Int J Epidemiol [Internet]. 2022 [cited 08/01/2026];50(6):1927-1935. Available from: https://doi.org/10.1093/ije/dyab153
26. World Medical Association. Ethical Principles for Medical Research Involving Human Subjects. Declaration of Helsinki [Internet]. Ferney-Voltaire: WMA; 2024 [cited 08/01/2026]. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
27. Ojeda Delgado L, Rodríguez Pino MY, Valladares Valle M, Díaz Yanes NM. Contribution of imaging studies to the diagnosis of breast cancer. Rev Finlay [Internet]. 2021 [cited 08/01/2026];11(4):423-435. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S2221-24342021000400423&lng=es
28. Lucas Choque A, Marín Macedo W. Knowledge about breast cancer and its correlation with the practice of breast self-examination in women of childbearing age attending the Dr. Osorio Pitta Surgical Medical Center [thesis]. Trujillo: Private University of the North; 2022 [cited 08/01/2026]. Available from: https://repositorio.upn.edu.pe/bitstream/handle/11537/32431/
29. Vargas Rodríguez M, Ponce Sanz AM, Reyes Reyes I, Rodríguez Morera M, Vilier Lores SA. Educational intervention on women with breast cancer risk factors at Office 8. In: III National Workshop and Conference for Residents and Health Professionals; 2024. [cited 08/01/2026]. Available from: https://jorcienciapdcl.sld.cu/index.php/jorgecienciapdcl2024/2024/paper/view/861/1157
30. Martínez Meza CM, Muñoz Sequeira MI, Parrales Baca DJ. Knowledge, attitudes and practices regarding breast cancer risk factors in patients treated at a Hospital in León, Nicaragua [thesis]. León: National Autonomous University of Nicaragua; 2025 [cited 08/01/2026]. Available from: http://riul.unanleon.edu.ni:8080/jspui/handle/123456789/10197
AUTHORSHIP CONTRIBUTION
LRBH: Conceptualization, content curation, investigation, methodology, administration, supervision, data collection, formal analysis (quantitative and qualitative), writing – original draft, review, and editing.
OGLN: Conceptualization, methodology, review, and editing.
IVG: Investigation, data collection.
LBS: Investigation, data collection.
LSC: Investigation, data collection.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING SOURCES
The authors received no funding for this article.
USE OF ARTIFICIAL INTELLIGENCE
The authors declare that no artificial intelligence was used in the writing of this manuscript.
Annex 1.
Patient Questionnaire. Mark with an X.
|
o Age (years) |
o <30 |
o 40-49 o 50-59 |
o 60-69 o ≥70 |
|
o Skin color |
o White |
o Black |
o Mestiza (Mixed-race) |
|
o Educational level |
o Primary school o Lower secondary school |
o Mid-level technician |
o Pre-university o University |
|
o First birth >30 years old |
o Yes |
o No |
o |
|
o Nulliparity |
o Yes |
o No |
o |
|
o Personal history |
o Ovarian cancer |
o Atypical hyperplasia |
o Breast cancer |
|
o First-line family history |
o Ovarian cancer |
o Colon cancer |
o Endometrial cancer |
|
o History of breast cancer in first-line relatives |
o Yes |
o No |
|
|
o Early menarche <10 years old |
o Yes |
o No |
|
|
o Late menopause >55 years old |
o Yes |
o No |
|
|
o Postmenopausal obesity (BMI >30) |
o Yes |
o No |
|
|
o Absence of breastfeeding or <3 months |
o Yes |
o No |
|
|
o Second-line family history of breast cancer |
o yes |
o No |
|
|
o Chronic non-communicable diseases |
o Arterial hypertension |
o Diabetes mellitus |
|
|
o Lifestyle |
o Smoking o Alcoholism |
o Sedentary lifestyle o Frequent stress |
|
|
o ¿Do you perform breast self-examination? |
o Yes |
o No |
|
|
o Knows the appropriate time for breast self-examination |
o Yes |
o No |
|
Annex 2
Informed Consent.
Date: _________
I: ___________________________________________, hereby approve my participation in the research being conducted, with the aim of identifying breast cancer risk factors at Family Medical Office No. 24 of the "José Jacinto Milanés" Polyclinic.
I have been informed:
· The objectives and benefits of the research, and that it does not represent any risk to my health.
· Participation is voluntary, and I may withdraw if I consider it appropriate, without this affecting the quality of medical care whenever I may require it.
· The information collected will only be used for scientific purposes.
Based on the above, I authorize my inclusion in the research study, and as proof thereof:
|
Patient's signature |
|
|
|
|
|
Witness's signature |
|
|
|
|
|
Investigator's signature |
|