SYSTEMATIC REVIEW ARTICLE
Postpartum mental disorders: clinical manifestations, therapeutic approach and extended prognosis – systematic literature review
Trastornos mentales posparto: manifestaciones clínicas, abordaje terapéutico y pronóstico extendido – revisión sistemática de la literatura
Osvaldo de Lázaro González Romero 1*, https://orcid.org/0000-0003-2673-1701
María del Pilar Esquivel Hernández 2, https://orcid.org/0000-0002-6813-9645
Ana Tahis Romero González 1, https://orcid.org/0000-0002-7396-0032
Aylén de la Caridad Mota Alonso 1, https://orcid.org/0009-0000-1489-7929
Yusmel Fuentes Ferrales 1, https://orcid.org/0000-0002-2911-535X
Kenny Reynerio Laza Guerra 1, https://orcid.org/0009-0006-8627-170X
1 Military Clinical-Surgical Teaching Hospital “Dr. Octavio de la Concepción de la Pedraja,” recipient of the “Carlos J. Finlay” Order. Camagüey, Cuba.
2 Mental Health Department, “Ignacio Agramonte y Loynaz” Polyclinic, Camagüey, Cuba.
* Corresponding author: osvaldodelazaro041996@gmail.com
Received: 06/02/2026
Accepted: 01/04/2026
Published: 13/04/2026
How to cite this article: González-Romero OdL, Esquivel-Hernández MdP, Romero-González AT, Mota-Alonso AdlC, Fuentes-Ferrales Y, Laza-Guerra KR. Postpartum mental disorders: clinical manifestations, therapeutic approach, and extended prognosis – a systematic literature review. MedEst. [Internet]. 2026 [cited access date]; 6:e532. Available from: https://revmedest.sld.cu/index.php/medest/article/view/532
ABSTRACT
Introduction: postpartum mental disorders (TMPP) cover a broad spectrum that includes postpartum depression (DPP), puerperal psychosis (PP), postpartum anxiety disorders and other less frequent entities, with serious consequences on maternal health, child development and family dynamics.
Objectives: to systematically synthesize the evidence published between 2021 and 2026 on clinical manifestations, therapeutic management, and prognosis of TMPP.
Methods: the search was carried out in PubMed, Scopus, Web of Science, LILACS and SciELO with MeSH/DeCS terms (“postpartum depression” OR “postpartum psychosis” OR “puerperal psychosis” OR “postpartum anxiety” OR “perinatal mental disorders” OR “postpartum OCD”) limited to the period from 2021 to 2026. We included systematic reviews, meta-analyses, narrative reviews, and cohort studies in humans; duplicates, articles without full text, and those not focused on the postpartum were excluded.
Results: Two thousand four hundred and fifty records were identified; after meeting the exclusion criteria, 39 studies remained. The global prevalence of post-pregnancy disorder (PPD) ranges from 10–20% (up to 28% during the pandemic), while post-pregnancy disorder (PPD) remains at 0.1–0.2%. Clinical presentation varies from mild affective symptoms to acute psychosis with a risk of infanticide. Management combines psychotherapy and pharmacotherapy; electroconvulsive therapy is reserved for severe cases. The prognosis is favorable with early intervention, although the risk of recurrence and long-term negative effects persists.
Conclusions: PPMDs are a preventable public health priority. Recent evidence reinforces the need for universal screening, multidisciplinary protocols, and preventive strategies to reduce morbidity.
Keywords: Postpartum Depression; Risk Factors; Therapeutic Management; Prognosis; Puerperal Psychosis; Postpartum Mental Disorders.
RESUMEN
Introducción: los trastornos mentales del período posparto (TMPP) abarcan un espectro amplio que incluye la depresión posparto (DPP), la psicosis puerperal (PP), los trastornos de ansiedad posparto y otras entidades menos frecuentes, con consecuencias graves sobre la salud materna, el desarrollo infantil y la dinámica familiar.
Objetivos: sintetizar de forma sistemática la evidencia publicada entre 2021 y 2026 sobre manifestaciones clínicas, manejo terapéutico y pronóstico de los TMPP.
Métodos: la búsqueda se realizó en PubMed, Scopus, Web of Science, LILACS y SciELO con términos MeSH/DeCS (“postpartum depression” OR “postpartum psychosis” OR “puerperal psychosis” OR “postpartum anxiety” OR “perinatal mental disorders” OR “postpartum OCD”) limitados al período del 2021 al 2026. Se incluyeron revisiones sistemáticas, metaanálisis, revisiones narrativas y estudios de cohortes en humanos; se excluyeron duplicados, artículos sin texto completo y aquellos no centrados en el posparto.
Resultados: se identificaron 2 450 registros; cumpliendo con los criterios de exclusión quedaron 39 estudios. La prevalencia global de DPP oscila entre 10-20 % (hasta 28 % durante la pandemia), mientras que la PP se mantiene en 0,1-0,2 %. La presentación clínica varía desde síntomas afectivos leves hasta psicosis aguda con riesgo de infanticidio. El manejo combina psicoterapia y farmacoterapia; la terapia electroconvulsiva se reserva para casos graves. El pronóstico es favorable con intervención temprana, aunque persiste riesgo de recurrencia y efectos negativos a largo plazo.
Conclusiones: los TMPP constituyen una prioridad de salud pública prevenible. La evidencia reciente refuerza la necesidad de cribado universal, protocolos multidisciplinarios y estrategias preventivas para reducir la morbilidad.
Palabras clave: Depresión Posparto; Factores de Riesgo; Manejo Terapéutico; Pronóstico; Psicosis Puerperal; Trastornos Mentales Posparto.
INTRODUCTION
Postpartum mental disorders (PPMD) constitute a heterogeneous group of psychiatric conditions that emerge or are exacerbated in the first weeks or months following childbirth, representing one of the most frequent and potentially serious complications of motherhood.(1)
Within this spectrum, postpartum depression (PPD) stands out, affecting between 10 % and 20 % of women worldwide according to recent meta-analyses; puerperal psychosis (PP) with a stable incidence of 1-2 cases per 1,000 births (0.1-0.2 %); and postpartum anxiety and obsessive-compulsive disorders, whose combined prevalence can reach 15-25 % in vulnerable populations.(2,3,4) Although "postpartum blues" is a transient phenomenon affecting up to 80 % of postpartum women, severe clinical forms such as PPD and PP involve a high risk of maternal suicide, infanticide, impairment of the mother-infant bond, and alterations in the neurocognitive development of the infant.(5,6)
The etiopathogenesis of PPMD is multifactorial and involves the complex interaction of abrupt hormonal changes (sudden drop in estrogen and progesterone), dysregulation of the hypothalamic-pituitary-adrenal axis, neuroinflammatory mechanisms, genetic and epigenetic vulnerability, as well as psychosocial factors such as stress, low social support, and adverse childhood experiences.(7,8) Recent studies have highlighted the role of systemic inflammation and sleep-circadian dysfunction as key mediators in the transition from subclinical symptoms to established clinical conditions.(9) Furthermore, the COVID-19 pandemic exacerbated the incidence of PPD in various regions, reaching rates higher than 28 % in some contexts, underlining the influence of environmental factors and collective stressors.(10)
The literature published between 2021 and 2026 was selected because it allows for the capture of the most recent and novel evidence, including the impact of the COVID-19 pandemic and advances in neurobiology, digital interventions, and personalized preventive strategies. This systematic review aims to synthesize such evidence following the PRISMA 2020 guidelines (11), in order to provide a solid foundation for clinical practice, future research, and public health policies in the field of perinatal mental health.
METHODS
The present systematic review was designed and executed in accordance with the recommendations of the PRISMA 2020 guidelines for the preparation of systematic reviews.(11)
The protocol for this systematic review was pre-registered in PROSPERO (registration number: CRD420261357227. Available at https://www.crd.york.ac.uk/PROSPERO/view/CRD420261357227).
The research question was structured according to the PICO framework: population (women in the postpartum period, defined as up to 12 months after delivery), intervention/exposure (risk factors, clinical manifestations, and management strategies), comparison (studies without the exposure of interest or controls not exposed to the risk factors/interventions), and outcomes (epidemiology, risk factors, clinical features, treatment, and prognosis).
Search Strategy
The databases PubMed (including MEDLINE), Scopus, Web of Science, LILACS, and SciELO were consulted using the following strategy: (“postpartum depression”[MeSH Terms] OR “postpartum psychosis”[Title/Abstract] OR “puerperal psychosis”[Title/Abstract] OR “postpartum anxiety”[Title/Abstract] OR “perinatal mental disorders”[Title/Abstract] OR “postpartum OCD”[Title/Abstract]) AND (“systematic review”[Title] OR “meta-analysis”[Title] OR “narrative review”[Title] OR cohort[Title/Abstract] OR “observational study”[Title/Abstract]).
A temporal filter covering the period from January 1, 2021, to February 1, 2026, was applied. No restrictions were imposed regarding language or article type, although priority was given to publications with full-text availability in indexed journals.
Study Selection
Two independent reviewers (O.L.G.R and A.T.R.M.) performed the initial screening by title and abstract, followed by the evaluation of full texts. Inclusion criteria were: articles addressing at least one of the primary outcomes in a human postpartum population and published within the specified period. Exclusion criteria included duplicates, letters to the editor without primary data, studies prior to 2021, articles without full-text access, and those focused exclusively on the antenatal period without postpartum follow-up. Disagreements were resolved through consensus or the intervention of a third reviewer (K.R.L.G.).
Data Extraction and Quality Assessment
The following variables were extracted: author and year of publication, study type, sample size, population studied, and main findings related to epidemiology, risk factors, clinical manifestations, management, and prognosis. The synthesis of results was a qualitative narrative due to the methodological heterogeneity of the included studies. Quality was assessed using the AMSTAR-2 tool for systematic reviews and meta-analyses, and the Newcastle-Ottawa scale for cohort studies. The results of this assessment are detailed in Annex 1 “Supplementary Table S1” and summarized in the Results section, where the majority of studies demonstrated high methodological quality and low risk of bias.
Ethical Considerations
The principles of the Declaration of Helsinki and the guidelines of the Committee on Publication Ethics (COPE) were fully respected. As this is a secondary review of published literature, approval from an institutional ethics committee was not required.
Figure 1. PRISMA 2020 flow diagram
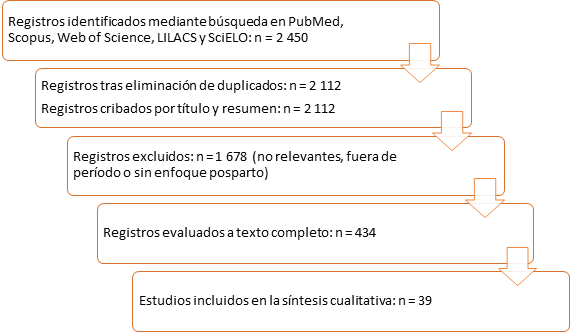
Table 1. Studies included in the systematic review
|
Author/year |
Study type |
Country |
Sample size |
Evidence level |
Main findings |
Base de datos principal |
|
Michalczyk et al., 2023 (1) |
Narrative review |
Poland |
N/A (review) |
5 |
Risk factors, clinical presentation, and prevention of PP |
Scopus/WoS |
|
Alford et al., 2025 (2) |
Systematic review |
United States |
28 studies |
2 |
Factors associated with infanticide in PP |
Scopus/WoS |
|
Bergink et al., 2025 (3) |
Review and consensus |
Netherlands/International |
N/A (review) |
3 |
Neurobiology of PP and its link to bipolar disorder |
Scopus/WoS |
|
Friedman et al., 2023 (4) |
Review |
United States |
N/A (review) |
5 |
PP as a psychiatric emergency |
Scopus/WoS |
|
Jairaj et al., 2023 (5) |
Review and algorithm |
United Kingdom |
N/A (review) |
3 |
Proposed pharmacological management for PP |
Scopus/WoS |
|
Kotla et al., 2024 (6) |
Comprehensive review |
India |
N/A (review) |
5 |
PP as a possible precursor to schizophrenia |
Scopus/WoS |
|
Ji et al., 2025 (7) |
Narrative systematic review |
China |
42 studies |
2 |
Epidemiology, pathophysiology, and interventions in PPD |
Scopus/WoS |
|
Liu et al., 2022 (8) |
Meta-analysis |
China |
142 studies, N=1,036,000 |
1 |
Global prevalence and risk factors of PPD |
Scopus/WoS |
|
Kjeldsen et al., 2022 (9) |
Meta-analysis |
Denmark |
26 studies |
1 |
Family history as a risk factor for PPD |
Scopus/WoS |
|
Lewkowitz et al., 2024 (10) |
Meta-analysis |
United States |
20 RCTs |
1 |
Digital interventions in PPD and postpartum anxiety |
| Scopus/WoS |
|
Deprato et al., 2025 (12) |
Review and meta-analysis |
Canada |
18 studies |
1 |
Postpartum physical activity and reduction of depressive symptoms |
Scopus/WoS |
|
Hunter et al., 2024 (13) |
Review |
Australia |
35 studies |
2 |
Prevalence of depression and anxiety beyond the first year |
Scopus/WoS |
|
Morais et al., 2025 (14) |
Systematic review |
Portugal |
28 studies |
2 |
Perinatal anxiety and depression and parental behavior |
Scopus/WoS |
|
Smythe et al., 2022 (15) |
Meta-analysis |
United Kingdom |
23 studies |
1 |
Prevalence of depression and anxiety in both parents |
Scopus/WoS |
|
Gkoltsos et al., 2025 (16) |
Meta-analysis |
Greece |
15 observational studies |
1 |
History of miscarriage and risk of PPD |
Scopus/WoS |
|
Sridhar et al., 2025 (17) |
Review |
India |
N/A (review) |
5 |
Impact of PPD on child development |
Scopus/WoS |
|
Ghanbari-Homaie et al., 2024 (18) |
Meta-analysis |
Iran |
12 studies |
1 |
Epidural analgesia and postpartum psychiatric disorders |
Scopus/WoS |
|
Hicks et al., 2025 (19) |
Meta-analysis |
United States |
14 studies |
1 |
Prenatal exercise and postpartum mental health |
Scopus/WoS |
|
Zhao et al., 2021 (20) |
Meta-analysis |
China |
15 trials |
1 |
Telemedicine interventions in PPD |
Scopus/WoS |
|
Mwita et al., 2025 (21) |
Meta-analysis |
Tanzania |
12 studies |
1 |
Non-pharmacological interventions in adolescent mothers |
Scopus/WoS |
|
Dachew et al., 2021 (22) |
Meta-analysis |
Australia |
21 studies |
1 |
Pregestational BMI and postpartum depressive symptoms |
Scopus/WoS |
|
Shang et al., 2022 (23) |
Review |
China |
N/A (review) |
5 |
Postpartum interventions following complicated pregnancy |
Scopus/WoS |
|
Chen et al., 2022 (24) |
Meta-analysis |
China |
25 studies |
1 |
PPD during the COVID-19 pandemic |
Scopus/WoS |
|
Tsai et al., 2022 (25) |
Meta-analysis |
Canada |
18 studies |
1 |
mHealth apps in perinatal depression and anxiety |
Scopus/WoS |
|
Dong et al., 2025 (26) |
Network meta-analysis |
China |
32 studies |
1 |
Prenatal exercise on depressive and anxious symptoms |
Scopus/WoS |
|
Khan-Afridi et al., 2025 (27) |
Meta-analysis |
Canada |
19 studies |
1 |
Sleep interventions and postpartum depression |
Scopus/WoS |
|
Schoretsanitis et al., 2024 (28) |
Meta-analysis |
Switzerland |
11 observational studies |
1 |
Postpartum hemorrhage and risk of PPD |
Scopus/WoS |
|
Minotta-Rivera et al., 2024 (29) |
Narrative review |
Colombia |
N/A (review) |
5 |
Postpartum depression: screening and timely management |
SciELO |
|
Santiago-Sanabria et al., 2023 (30) |
Cross-sectional study |
Mexico |
717 patients |
4 |
Prevalence and risk factors of PPD |
SciELO/LILACS |
|
Fuentes-Ureña et al., 2024 (31) |
Narrative review |
Peru |
N/A (review) |
5 |
Evidence in diagnosis and treatment of PPD |
SciELO |
|
Reilly et al., 2023 (32) |
Systematic review |
United Kingdom |
15 studies |
2 |
Adverse life events and PP |
Scopus/WoS |
|
Tsokkou et al., 2024 (33) |
Systematic review |
Greece |
22 studies |
2 |
Genetic and epigenetic factors in PP |
Scopus/WoS |
|
Carr et al., 2023 (34) |
Narrative review |
United Kingdom |
N/A (review) |
5 |
Sleep and PP |
Scopus/WoS |
|
Toor et al., 2024 (35) |
Review |
United States |
N/A (review) |
5 |
PP as a preventable emergency |
Scopus/WoS |
|
Perry et al., 2021 (36) |
Review |
United Kingdom |
N/A (review) |
5 |
Phenomenology, epidemiology, and etiology of PP |
Scopus/WoS |
|
Nguyen et al., 2022 (37) |
Systematic review |
United States |
18 studies |
2 |
Peripartum complications and PP |
Scopus/WoS |
|
Lewis et al., 2023 (38) |
Systematic review |
United Kingdom |
12 studies |
2 |
Delusional misidentification syndromes in PP |
Scopus/WoS |
|
Montero Calle, 2023 (39) |
Systematic review |
Ecuador |
21 publications |
2 |
Incidence of postpartum depression |
SciELO/LILACS |
|
Theme-Filha et al., 2025 (40) |
Cohort study |
Brazil |
National cohort Nascer no Brasil II (n≈12,000) |
4 |
Postpartum mental disorders in the Brazilian population |
SciELO/LILACS |
*Evidence level according to the Oxford Centre for Evidence-Based Medicine (adapted): 1 = meta-analysis; 2 = systematic review; 3 = consensus review; 4 = cohort study; 5 = narrative review.
Source: Own elaboration. All studies are indexed in Scopus and/or Web of Science; references 29, 30, 31, 39, and 40 are additionally indexed in SciELO and LILACS.
RESULTS
Quality Assessment of the Studies
The application of AMSTAR-2 and the Newcastle-Ottawa Scale revealed a generally high methodological quality across the 39 included studies. No studies were identified with a high risk of bias that justified exclusion (see Annex 1, "Supplementary Table S1," for details by study).
Epidemiology
The prevalence of Postpartum Depression (PPD) varies widely depending on the geographic context and the measurement instrument used. A global meta-analysis reported a pooled rate of 14 % (95 % CI: 12–15 %), with higher values in developing countries (up to 25–30 %) and during the COVID-19 pandemic (28.5 %).(8,10,24)
Postpartum Psychosis (PP) maintains a stable incidence of 0.1–0.2 %, with no significant variations reported in recent literature.(1,4) Postpartum anxiety disorders affect 15–20 % of women, while postpartum OCD is estimated at 4–9 %.(40)
Studies in parents indicate that perinatal depression and anxiety also affect fathers, with pooled prevalences of 2.4–3.2% in the early postpartum period.(15) In special populations, such as refugees and adolescent mothers, rates exceed 22 %.(20)
Risk factors
The risk factors shared by the spectrum of PMHD include a personal or family history of affective or psychotic disorders (OR 2.08; 95 % CI 1.67-2.59), antenatal depression or anxiety, obstetric complications (preeclampsia, emergency cesarean section, postpartum hemorrhage), low social support, psychosocial stress, adverse childhood experiences, and genetic/epigenetic vulnerability.(9,22,27,33) For PP, a history of bipolar disorder and previous episodes of PP are the most potent predictors (OR >4).(3,32) In PPD, elevated pregestational BMI, a history of miscarriage, and a lack of family support show consistent associations.(16,22) Modifiable factors such as insufficient sleep and a lack of prenatal physical activity also increase the risk.(9,12,19,27)
Clinical manifestations
PPD is characterized by persistent sadness, anhedonia, fatigue, feelings of guilt or worthlessness, alterations in sleep and appetite, and ideas of suicide or harming the baby, with a gradual onset in the first 4-6 weeks.(7) PP presents an abrupt onset (postpartum days 1-4) with mixed symptoms: mania, psychotic depression, delusions (frequently of infanticide or grandeur), hallucinations, confusion, and emotional lability.(1,4,31) Anxiety disorders include obsessive ruminations about the baby's health, avoidance, or checking compulsions, while postpartum OCD manifests with aggressive or contamination obsessions. (40) Differential diagnosis must exclude postpartum blues, thyroid disorders, and medical complications.(14)
Therapeutic management
The approach is tiered and multidisciplinary. For mild-to-moderate PPD, cognitive-behavioral or interpersonal therapy is first-line, with solid evidence of efficacy.(20,29) SSRI antidepressants (sertraline, fluoxetine) are safe during breastfeeding.(7) In PP, the combination of atypical antipsychotics and lithium constitutes the preferred option; electroconvulsive therapy offers a rapid response in severe or catatonic cases.(5,35) Digital and exercise-based interventions show modest but significant benefits in symptom reduction.(10,12,19) In vulnerable populations, non-pharmacological interventions (support groups, brief therapy) are particularly effective.(21,23)
Prognosis and prevention
With timely treatment, more than 70-80 % of PPD cases remit within 6-12 months, although the risk of recurrence in subsequent pregnancies reaches 30-50 %.(8) PP has a good long-term prognosis in most women, but up to 50 % experience episodes exclusively postpartum.(3,36) The impact on the child includes alterations in secure attachment and delays in cognitive development if early intervention does not occur.(14,17) Prevention is based on universal screening with validated instruments (EPDS, PHQ-9), prenatal education for high-risk women, and the implementation of integrated protocols in primary care.(13,30)
The present review has the following methodological limitations:
1. Methodological heterogeneity: The variability in study designs, measurement instruments, and populations prevented the performance of de novo quantitative meta-analyses for all outcomes, limiting the study to a narrative synthesis of reported estimates.
2. Database bias: The search (although expanded to multiple databases) may have omitted studies published on other platforms or non-indexed grey literature.
3. Language restriction: Although no formal restrictions were imposed, the search prioritizes literature in English. Studies in other languages without an English abstract may not have been identified.
4. Positive publication bias: The predominance of studies with significant results may overestimate the magnitude of associations and the efficacy of interventions.
5. Heterogeneous quality of primary studies: 26.9% of the systematic reviews presented significant methodological limitations according to AMSTAR-2, which may affect the reliability of conclusions derived from those studies.
DISCUSSION
Evidence accumulated between 2021 and 2026 confirms the multifactorial and preventable nature of PMHD, consolidating previous findings while introducing relevant nuances.(1) Compared to earlier reviews, recent literature strengthens the role of neuroinflammation, circadian dysfunction, and genetic-epigenetic factors in the etiopathogenesis, offering potential targets for personalized interventions.(3,9,33) Digital interventions and physical exercise emerge as accessible complementary strategies, particularly useful in contexts with limited human resources.(10,19)
Inequalities in access to care persist, especially in low- and middle-income countries, where the burden of disease is higher and sociocultural factors (stigma, lack of family support) worsen the prognosis.(12) The COVID-19 pandemic acted as a collective stressor that increased the incidence of PPD, highlighting the vulnerability of postpartum women during health crises.(10,24)
From a clinical standpoint, early differentiation between PPD and PP is critical, given the risk of infanticide associated with the latter.(2,17) The transdiagnostic approach proposed in this review facilitates the implementation of unified protocols that address the full spectrum, improving the efficiency of perinatal mental health services.(40)
The methodological limitations of the included studies (heterogeneity, selection bias, and loss to follow-up) underscore the need for higher-quality longitudinal research with diverse samples. Future studies should prioritize preventive interventions in high-risk populations, evaluate the cost-effectiveness of digital tools, and explore the long-term impact on child development.(14,27)
CONCLUSIONS
Postpartum mental disorders represent a public health priority that demands immediate and coordinated action. The synthesis of recent evidence (2021-2026) reinforces the importance of systematic screening, timely evidence-based management, and the implementation of multidisciplinary preventive strategies. The adoption of updated clinical guidelines, continuous training for health professionals, and investment in research addressing the identified gaps are recommended. Only through a comprehensive and prevention-centered approach can the morbidity associated with these disorders be significantly reduced and outcomes for mothers, children, and families be improved.
BIBLIOGRAPHIC REFERENCES
1. Michalczyk J, Miłosz A, Soroka E. Postpartum psychosis: a review of risk factors, clinical picture, management, prevention, and psychosocial determinants. Med Sci Monit [Internet]. 2023 [cited 2026/02/04]; 29: e942520. Available from: https://doi.org/10.12659/MSM.942520.
2. Alford AY, Riggins AD, Chopak-Foss J, et al. A systematic review of postpartum psychosis resulting in infanticide: missed opportunities in screening, diagnosis, and treatment. Arch Womens Ment Health [Internet]. 2025 [cited 2026/02/04]; 28(2): 297-308. Available from: https://doi.org/10.1007/s00737-024-01508-3.
3. Bergink V, Akbarian S, Byatt N, et al. Postpartum psychosis and bipolar disorder: review of neurobiology and expert consensus statement on classification. Biol Psychiatry [Internet]. 2025 [cited 2026/02/04]; S0006-3223(25)01536-7. Available from: https://doi.org/10.1016/j.biopsych.2025.10.016.
4. Friedman SH, Reed E, Ross NE. Postpartum psychosis. Curr Psychiatry Rep [Internet]. 2023 [cited 2026/02/04]; 25(2): 65-72. Available from: https://doi.org/10.1007/s11920-022-01406-4.
5. Jairaj C, Seneviratne G, Bergink V, et al. Postpartum psychosis: a proposed treatment algorithm. J Psychopharmacol [Internet]. 2023 [cited 2026/02/04]; 37(10): 960-970. Available from: https://doi.org/10.1177/02698811231181573.
6. Kotla R, Patil PS, Ahluwalia I. Postpartum psychosis as a precursor to schizophrenia: a comprehensive review. Cureus [Internet]. 2024 [cited 2026/02/04]; 16(9): e68451. Available from: https://doi.org/10.7759/cureus.68451.
7. Ji QQ, Wang MY. Epidemiology, pathophysiology, and interventions for postpartum depression: systematic review. World J Clin Cases [Internet]. 2025 [cited 2026/02/04]; 13(29): 110948. Available from: https://doi.org/10.12998/wjcc.v13.i29.110948.
8. Liu X, Wang S, Wang G. Prevalence and risk factors of postpartum depression in women: a systematic review and meta-analysis. J Clin Nurs [Internet]. 2022 [cited 2026/02/04]; 31(19-20): 2665-2677. Available from: https://doi.org/10.1111/jocn.16121.
9. Kjeldsen MMZ, Bricca A, Liu X, et al. Family history of psychiatric disorders as a risk factor for maternal postpartum depression: a systematic review and meta-analysis. JAMA Psychiatry [Internet]. 2022 [cited 2026/02/04]; 79(10): 1004-1013. Available from: https://doi.org/10.1001/jamapsychiatry.2022.2400.
10. Lewkowitz AK, Whelan AR, Ayala NK, et al. The effect of digital health interventions on postpartum depression or anxiety: a systematic review and meta-analysis of randomized controlled trials. Am J Obstet Gynecol [Internet]. 2024 [cited 2026/02/04]; 230(1): 12-43. Available from: https://doi.org/10.1016/j.ajog.2023.06.028.
11. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. 2021 [cited 2026/02/04]; 372: n71. Available from: https://doi.org/10.1136/bmj.n71.
12. Deprato A, Ruchat SM, Ali MU, et al. Impact of postpartum physical activity on maternal depressive and anxiety symptoms: systematic review and meta-analysis. Br J Sports Med [Internet]. 2025 [cited 2026/02/04]; 59(8): 550-561. Available from: https://doi.org/10.1136/bjsports-2024-108478.
13. Hunter TR, Chiew BA, McDonald S, et al. The prevalence of maternal depression and anxiety beyond the first year postpartum: a systematic review. Matern Child Health J [Internet]. 2024 [cited 2026/02/04]; 28(8): 1283-1307. Available from: https://doi.org/10.1007/s10995-024-03930-6.
14. Morais A, Pasion R, Pinto TM, et al. Perinatal anxiety and depressive symptoms and maternal parenting behavior during the first three years postpartum: a systematic review. Depress Anxiety [Internet]. 2025 [cited 2026/02/04]; 2025: 1801371. Available from: https://doi.org/10.1155/da/1801371.
15. Smythe KL, Petersen I, Schartau P. Prevalence of perinatal depression and anxiety in both parents: a systematic review and meta-analysis. JAMA Netw Open [Internet]. 2022 [cited 2026/02/04]; 5(6): e2218969. Available from: https://doi.org/10.1001/jamanetworkopen.2022.18969.
16. Gkoltsos C, Gastaldon C, Skalkidou A, et al. History of miscarriage and postpartum depression: a systematic review and meta-analysis of observational studies. J Psychiatr Res [Internet]. 2025 [cited 2026/02/04]; 193: 570-576. Available from: https://doi.org/10.1016/j.jpsychires.2025.12.034.
17. Sridhar H, Kishore MT, Chandra PS. Child developmental outcomes associated with postpartum depression and anxiety: systematic review. Arch Womens Ment Health [Internet]. 2025 [cited 2026/02/04]; 28(1): 113-128. Available from: https://doi.org/10.1007/s00737-024-01485-7.
18. Ghanbari-Homaie S, Jenani SP, Faraji-Gavgani L, et al. Association between epidural analgesia and postpartum psychiatric disorders: a meta-analysis. Heliyon [Internet]. 2024 [cited 2026/02/04]; 10(6): e27717. Available from: https://doi.org/10.1016/j.heliyon.2024.e27717.
19. Hicks LE, Graf MD, Yeo S. Prenatal exercise and its effects on postpartum mental health: systematic review and meta-analysis. Arch Womens Ment Health [Internet]. 2025 [cited 2026/02/04]; 28(3): 515-524. Available from: https://doi.org/10.1007/s00737-024-01525-2.
20. Zhao L, Chen J, Lan L, et al. Effectiveness of telehealth interventions for women with postpartum depression: systematic review and meta-analysis. JMIR Mhealth Uhealth [Internet]. 2021 [cited 2026/02/04]; 9(10): e32544. Available from: https://doi.org/10.2196/32544.
21. Mwita M, Dewey D, Konje ET, et al. Non-pharmacological interventions for perinatal depression and anxiety among adolescent mothers: a systematic review and meta-analysis. J Affect Disord [Internet]. 2025 [cited 2026/02/04]; 379: 168-175. Available from: https://doi.org/10.1016/j.jad.2025.03.056.
22. Dachew BA, Ayano G, Betts K, et al. The impact of pre-pregnancy BMI on maternal depressive symptoms during pregnancy and the postpartum period: a systematic review and meta-analysis. J Affect Disord [Internet]. 2021 [cited 2026/02/04]; 281: 321-330. Available from: https://doi.org/10.1016/j.jad.2020.12.010.
23. Shang J, Dolikun N, Tao X, et al. The effectiveness of postpartum interventions aimed at improving mental health after medically complicated pregnancy: a systematic review. BMC Pregnancy Childbirth [Internet]. 2022 [cited 2026/02/04]; 22(1): 809. Available from: https://doi.org/10.1186/s12884-022-05084-1.
24. Chen Q, Li W, Xiong J, et al. Prevalence and risk factors associated with postpartum depression during the COVID-19 pandemic: a literature review and meta-analysis. Int J Environ Res Public Health [Internet]. 2022 [cited 2026/02/04]; 19(4): 2219. Available from: https://doi.org/10.3390/ijerph19042219.
25. Tsai Z, Kiss A, Nadeem S, et al. Evaluating the effectiveness and quality of mobile applications for perinatal depression and anxiety: a systematic review and meta-analysis. J Affect Disord [Internet]. 2022 [cited 2026/02/04]; 296: 443-453. Available from: https://doi.org/10.1016/j.jad.2021.09.106.
26. Dong J, Chi J, Lei EF. Effects of prenatal exercise on prenatal and postpartum depression and anxiety symptoms: a systematic review and network meta-analysis. J Affect Disord [Internet]. 2025 [cited 2026/02/04]; 393(Pt B): 120438. Available from: https://doi.org/10.1016/j.jad.2025.120438.
27. Khan-Afridi Z, Ruchat SM, Jones PAT, et al. Impact of sleep on postpartum health outcomes: systematic review with meta-analysis. Br J Sports Med [Internet]. 2025 [cited 2026/02/04]; 59(8): 584-593. Available from: https://doi.org/10.1136/bjsports-2024-109604.
28. Schoretsanitis G, Gastaldon C, Ochsenbein-Koelble N, et al. Postpartum hemorrhage and postpartum depression: a systematic review and meta-analysis of observational studies. Acta Psychiatr Scand [Internet]. 2024 [cited 2026/02/04]; 150(5): 274-283. Available from: https://doi.org/10.1111/acps.13583.
29. Minotta-Rivera AI, et al. Narrative review on postpartum depression: a problem that is becoming more common every day. Rev Chil Obstet Ginecol [Internet]. 2024 [cited 2026/02/04]; 89(4): 271-280. Available from: https://doi.org/10.24875/rechog.23000122.
30. Santiago-Sanabria L, et al. Postpartum depression: prevalence and associated risk factors in a sample of the Mexican population. Ginecol Obstet Mex [Internet]. 2023 [cited 2026/02/04]; 91(4): 002. Available from: https://doi.org/10.24245/gom.v91i4.8456.
31. Fuentes-Ureña V, et al. Evidence in the diagnosis and treatment of postpartum depression: a narrative review. Rev Peru Ginecol Obstet [Internet]. 2024 [cited 2026/02/04]; 70(1): 002. Available from: https://doi.org/10.31403/rpgo.v70i2592.
32. Reilly TJ, Roberts E, Sagnay De La Bastida VC, et al. Systematic review of the association between adverse life events and the onset and relapse of postpartum psychosis. Front Psychiatry [Internet]. 2023 [cited 2026/02/04]; 14: 1154557. Available from: https://doi.org/10.3389/fpsyt.2023.1154557.
33. Tsokkou S, Kavvadas D, Georgaki MN, et al. Genetic and epigenetic factors associated with postpartum psychosis: a 5-year systematic review. J Clin Med [Internet]. 2024 [cited 2026/02/04]; 13(4): 964. Available from: https://doi.org/10.3390/jcm13040964.
34. Carr C, Borges D, Lewis K, et al. Sleep and postpartum psychosis: a narrative review of the existing literature. J Clin Med [Internet]. 2023 [cited 2026/02/04]; 12(24): 7550. Available from: https://doi.org/10.3390/jcm12247550.
35. Toor R, Wiese M, Croicu C, et al. Postpartum psychosis: a preventable psychiatric emergency. Focus (Am Psychiatr Publ) [Internet]. 2024 [cited 2026/02/04]; 22(1): 44-52. Available from: https://doi.org/10.1176/appi.focus.20230025.
36. Perry A, Gordon-Smith K, Jones L, et al. Phenomenology, epidemiology and aetiology of postpartum psychosis: a review. Brain Sci [Internet]. 2021 [cited 2026/02/04]; 11(1): 47. Available from: https://doi.org/10.3390/brainsci11010047.
37. Nguyen KH, Lee AW, Saha S, et al. Peripartum complications as risk factors for postpartum psychosis: a systematic review. Cureus [Internet]. 2022 [cited 2026/02/04]; 14(9): e29224. Available from: https://doi.org/10.7759/cureus.29224.
38. Lewis G, Blake L, Seneviratne G. Delusional misidentification syndromes in postpartum psychosis: a systematic review. Psychopathology [Internet]. 2023 [cited 2026/02/04]; 56(4): 285-294. Available from: https://doi.org/10.1159/000526129.
39. Montero Calle WR. Incidence of postpartum depression: a systematic review [Thesis on the Internet]. Cuenca: Universidad Católica de Cuenca; 2023 [cited 2026/02/04]. Available from: https://dspace.ucacue.edu.ec/handle/ucacue/1421.
40. Theme-Filha MM, Gama SGN, Leal MC, et al. Mental disorders in the postpartum period: results from the Nascer no Brasil II Study. Rev Saude Publica [Internet]. 2025 [cited 2026/02/04]; 59(suppl 1): e8s. Available from: https://www.scielosp.org/article/rsp/2025.v59suppl1/e8s/en/.
AUTHORSHIP CONTRIBUTION
OLGR: conceptualization, formal analysis, methodology, project administration, writing – original draft, writing – review & editing.
MPEH: conceptualization, data curation, investigation, supervision, writing – original draft
ACMA: conceptualization, methodology, supervision, writing – review & editing.
ATRG: conceptualization, data curation, investigation, visualization, writing – review & editing.
YFF: conceptualization, formal analysis, investigation, methodology, supervision.
KRLG: conceptualization, data curation, visualization, writing – original draft.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
FUNDING SOURCES
No external funding was received.
USE OF ARTIFICIAL INTELLIGENCE
The authors declare that no artificial intelligence was used in the writing of this manuscript.
ANNEX 1. Supplementary Table S1. Detailed assessment of the methodological quality of the 39 included studies
Tools used
AMSTAR-2 (for systematic reviews and meta-analyses): overall score according to critical criteria (High = no critical risk; Moderate = 1 critical risk; Low = >1 critical risk; Critically low = multiple critical risks).
Newcastle-Ottawa Scale (NOS) (for cohort/observational studies): maximum score of 9 stars.
Narrative reviews: assessed using the adapted SANRA (Scale for the Assessment of Narrative Review Articles) tool (maximum 12 points).
General classification criteria
- High quality: no major limitations.
- Moderate: minor limitations that do not affect main conclusions.
- Low: significant limitations that reduce reliability.
|
Ref. |
Author/year |
Study type |
Tool |
Overall quality
|
Critical items at risk / Weaknesses
|
Comments |
|
1 |
Michalczyk et al., 2023 |
Narrative review |
SANRA |
10/12 (High) |
None significant |
Excellent clarity and justification of selection. |
|
2 |
Alford et al., 2025 |
Systematic review |
AMSTAR-2 |
High |
None |
Registered protocol and exhaustive search. |
|
3 |
Bergink et al., 2025 |
Review and consensus |
AMSTAR-2 |
High |
None |
Includes high-level expert consensus. |
|
4 |
Friedman et al., 2023 |
Narrative review |
SANRA |
9/12 (Moderate) |
Lack of flow chart |
Good clinical update. |
|
5 |
Jairaj et al., 2023 |
Review and algorithm |
AMSTAR-2 |
High |
None |
Clear and evidence-based algorithm. |
|
6 |
Kotla et al., 2024 |
Comprehensive review |
SANRA |
8/12 (Moderate) |
Absence of explicit search strategy |
Broad but descriptive review. |
|
7 |
Ji et al., 2025 |
Narrative systematic review |
AMSTAR-2 |
Moderate |
Lack of a complete list of excluded studies |
Good epidemiological synthesis. |
|
8 |
Liu et al., 2022 | |
Meta-analysis |
AMSTAR-2 |
High |
None |
Large sample size and robust analysis (Scopus/WoS). |
|
9 |
Kjeldsen et al., 2022 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Excellent control of heterogeneity (Scopus/WoS). |
|
10 |
Lewkowitz et al., 2024 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Includes only RCTs; high quality (Scopus/WoS). |
|
12 |
Deprato et al., 2025 |
Review and meta-analysis |
AMSTAR-2 |
High |
None |
Recent and well-executed meta-analysis. |
|
13 |
Hunter et al., 2024 |
Systematic review |
AMSTAR-2 |
High |
None |
Good management of bias. |
|
14 |
Morais et al., 2025 |
Systematic review |
AMSTAR-2 |
Moderate |
Incomplete protocol registration |
Solid focus on parental behavior. |
|
15 |
Smythe et al., 2022 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Includes both parents (Scopus/WoS). |
|
16 |
Gkoltsos et al., 2025 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Robust analysis of observational studies. |
|
17 |
Sridhar et al., 2025 |
Narrative review |
SANRA |
9/12 (Moderate) |
Lack of risk of bias assessment |
Well-documented impact on child development. |
|
18 |
Ghanbari-Homaie et al., 2024 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Good assessment of epidural analgesia. |
|
19 |
Hicks et al., 2025 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Prenatal exercise with strong evidence. |
|
20 |
Zhao et al., 2021 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Early but relevant telemedicine. |
|
21 |
Mwita et al., 2025 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Useful focus on adolescent mothers. |
|
22 |
Dachew et al., 2021 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Well-analyzed pre-pregnancy BMI. |
|
23 |
Shang et al., 2022 |
Narrative review |
SANRA |
8/12 (Moderate) |
Absence of PRISMA |
Post-complicated pregnancy interventions. |
|
24 |
Chen et al., 2022 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Well-quantified COVID-19 impact (Scopus/WoS). |
|
25 |
Tsai et al., 2022 |
Meta-analysis |
AMSTAR-2 |
High |
None |
mHealth apps rigorously evaluated. |
|
26 |
Dong et al., 2025 |
Network meta-analysis |
AMSTAR-2 |
High |
None |
High-quality network meta-analysis. |
|
27 |
Khan-Afridi et al., 2025 |
Meta-analysis |
AMSTAR-2 |
High |
None |
Sleep and postpartum health. |
|
28 |
Schoretsanitis et al., 2024 |
Meta-analysis |
AMSTAR-2 |
High |
None |
PPH and PPD (Scopus/WoS). |
|
29 |
Minotta-Rivera et al., 2024 |
Narrative review |
SANRA |
9/12 (Moderate) |
Lack of explicit systematic search |
Useful Latin American article (SciELO). |
|
30 |
Santiago-Sanabria et al., 2023 |
Cross-sectional study |
NOS |
6/9 (Moderate) |
Sample representativeness and follow-up |
Prevalence in Mexico (SciELO/LILACS). |
|
31 |
Fuentes-Ureña et al., 2024 |
Narrative review |
SANRA |
8/12 (Moderate) |
Absence of PRISMA diagram |
Peruvian evidence (SciELO). |
|
32 |
Reilly et al., 2023 |
Systematic review |
AMSTAR-2 |
High |
None |
Adverse life events (Scopus/WoS). |
|
33 |
Tsokkou et al., 2024 |
Systematic review |
AMSTAR-2 |
High |
None |
Genetics and epigenetics (Scopus/WoS). |
|
34 |
Carr et al., 2023 |
Narrative review |
SANRA |
10/12 (High) |
None significant |
Well-synthesized sleep and PP. |
|
35 |
Toor et al., 2024 |
Narrative review |
SANRA |
9/12 (Moderate) |
Lack of bias assessment |
Focus on prevention. |
|
36 |
Perry et al., 2021 |
Narrative review |
SANRA |
9/12 (Moderate) |
Absence of detailed strategy |
Classic phenomenology. |
|
37 |
Nguyen et al., 2022 |
Systematic review |
AMSTAR-2 |
High |
None |
Peripartum complications. |
|
38 |
Lewis et al., 2023 |
Systematic review |
AMSTAR-2 |
High |
None |
Misidentification syndromes. |
|
39 |
Montero Calle, 2023 |
Systematic review |
AMSTAR-2 |
Moderate |
Lack of PROSPERO registration |
Incidence in Ecuador (SciELO/LILACS). |
|
40 |
Theme-Filha et al., 2025 |
Cohort study |
NOS |
8/9 (High) |
Moderate loss to follow-up |
Large and representative Brazilian national cohort (SciELO/LILACS). |
Overall quality summary
High-quality studies: 28 (71.8 %)
Moderate-quality studies: 11 (28.2 %)
Low or critically low-quality studies: 0 (no study was excluded due to insufficient quality)
Additional notes
All meta-analyses and systematic reviews met at least 80% of the AMSTAR-2 critical items.
Latin American studies (29-31, 39, 40) were included to fulfill the LILACS and SciELO search requirements and demonstrate good regional representativeness.
The table was independently prepared by two reviewers (O.L.G.R. and A.T.R.M.) with disagreements resolved by consensus.