ORIGINAL ARTICLE
Effectiveness of laser therapy in patients with cervical pain syndrome: a study in a rehabilitation service, Matanzas
Efectividad de la laserterapia en pacientes con síndrome doloroso cervical: estudio en servicio de rehabilitación, Matanzas
Laura María Herrera Fraga 1*, https://orcid.org/0009-0004-8565-152X
Jayne Bárbara Peñate Brito 2, https://orcid.org/0000-0002-0872-1692
Gladys García Peñate 1, https://orcid.org/0009-0009-6156-5009
Narciso Feliciano Martínez Díaz 3, https://orcid.org/0009-0000-9150-3065
Idalia Teresita Hernández Hervis 1, https://orcid.org/0000-0002-5772-2034
Miriela Diago Rodríguez 4, https://orcid.org/0009-0002-8088-7627
¹ Faustino Pérez Provincial Clinical Surgical Teaching Hospital. Matanzas, Cuba.
² “José Jacinto Milanés” Polyclinic. Matanzas, Cuba.
3 Samuel Fernández Polyclinic. Matanzas, Cuba.
4 General Directorate of Health. Provincial Department of Rehabilitation. Matanzas, Cuba.
* Corresponding author: lherrera.mtz@infomed.sld.cu
Received: 25/01/2025
Accepted: 01/07/2025
How to cite this article: Herrera-Fraga LM, Peñate-Brito JB, García-Peñate G, Martínez-Díaz NF, Hernández-Hervis IT, Diago-Rodríguez M. Effectiveness of laser therapy in patients with cervical pain syndrome: a study in a rehabilitation service, Matanzas. MedEst. [Internet]. 2025 [cited access date]; 5:e402. Available in: https://revmedest.sld.cu/index.php/medest/article/view/402
ABSTRACT
Introduction: cervical pain syndrome is a common reason for consultation and is considered one of the most common spinal pain conditions. The use of low-level lasers in the treatment of spinal disorders is poorly understood.
Objective: to evaluate the effectiveness of laser therapy in patients with cervical pain syndrome in a rehabilitation service in Matanzas.
Methods: an experimental, longitudinal, and prospective study 38 patients were randomly divided into two groups: one received laser therapy + cryotherapy and the other NSAIDs + cryotherapy. Pain intensity was measured using the Visual Analog Scale (VAS) and the Likert scale, and functional disability was measured using the Neck Disability Index (NDI) at the beginning and end of treatment.
Results: Laser therapy significantly outperformed NSAIDs 52,4 % of patients were pain-free (vs. 17,7 % with NSAIDs) and showed significantly greater functional improvement (33,3 % without disability vs. 5,9 %). Its overall effectiveness was 76,2 % and required fewer treatment sessions. The main risk factors were poor postural habits (84,2 %) and physical inactivity (76,3 %).
Conclusions: Laser therapy combined with cryotherapy was shown to be more effective and faster than treatment with NSAIDs and cryotherapy in relieving pain and improving functionality in patients with acute and subacute neck pain, positioning it as a superior therapeutic alternative.
Keywords: Neck Pain; Laser Therapy; Cryotherapy; Acute Pain; Rehabilitation; Ibuprofen
RESUMEN
Introducción: el síndrome doloroso cervical constituye un frecuente motivo de consulta y está considerado como una de las entidades dolorosas más frecuentes de la columna vertebral. La aplicación de láser de baja potencia en el tratamiento de los desórdenes de columna es poco conocida.
Objetivo: evaluar la efectividad de la laserterapia en pacientes con síndrome doloroso cervical en un servicio de rehabilitación en Matanzas.
Métodos: estudio experimental, longitudinal y prospectivo. Se dividió aleatoriamente a 38 pacientes en dos grupos: uno recibió laserterapia + crioterapia y el otro AINEs + crioterapia. La intensidad del dolor se midió con la Escala Visual Analógica (EVA) y la escala de Likert, y la discapacidad funcional con el Neck Disability Index (NDI), al inicio y al final del tratamiento.
Resultados: la laserterapia superó significativamente a los AINEs. Un 52,4 % de pacientes quedaron sin dolor (frente al 17,7 % con AINEs) y mostró una mejora funcional muy superior (33,3 % sin discapacidad vs. 5,9 %). Su efectividad global fue del 76,2 % y requirió menos sesiones de tratamiento. Los principales factores de riesgo fueron los malos hábitos posturales (84,2 %) y la inactividad física (76,3 %).
Conclusiones: la laserterapia combinada con crioterapia demostró ser más efectiva y rápida que el tratamiento con AINEs y crioterapia para aliviar el dolor y mejorar la funcionalidad en pacientes con cervicalgia aguda y subaguda, posicionándose como una alternativa terapéutica superior.
Palabras Clave: Cervicalgia; Laserterapia; Crioterapia; Dolor Agudo; Rehabilitación; Ibuprofeno
INTRODUCTION
Cervical pain syndrome, or mechanical neck pain, is one of the most prevalent musculoskeletal conditions worldwide, affecting approximately 528 million people. It is most prevalent among women (60 %) and those over 55 years of age (73 %). (1)
This condition constitutes a significant public health problem due to its negative impact on quality of life, limited personal autonomy, and considerable socioeconomic repercussions resulting from work absenteeism and associated healthcare costs. (2,3)
The pathophysiology of neck pain involves complex neurophysiological mechanisms that include local inflammatory processes, peripheral and central sensitization, and cervical muscle dysfunction. (4) According to the Quebec Task Force on Spinal Disorders classification, mechanical neck pain predominantly falls into diagnostic categories 1 and 2 (neck pain with or without proximal radiation) (5), typically progressing through acute (<4 weeks), subacute (4–12 weeks), and chronic (>12 weeks) phases. (6)
Conventional therapeutic management includes various modalities such as thermotherapy, electrotherapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and active and passive physiotherapy approaches. (7,8) However, the efficacy of these interventions shows variable results, with inconsistent therapeutic responses and potential adverse effects associated with prolonged NSAID use, particularly at the gastrointestinal level. (9,10) This therapeutic limitation underscores the urgent need to explore and validate safe and effective alternative interventions.
Low-level laser therapy (LLLT) or photobiomodulation is emerging as a promising therapeutic modality within physical medicine and rehabilitation. Its mechanism of action is based on photonic interaction with mitochondrial chromophores, primarily cytochrome c oxidase, triggering a cascade of biochemical events that include increased adenosine triphosphate (ATP) synthesis, modulation of reactive oxygen species, reduction of proinflammatory markers (TNF-α, IL-1β, COX-2), and stimulation of local microcirculation. (11,12) These effects are clinically translated into documented analgesic, anti-inflammatory, and trophic actions. (13,14)
Current evidence suggests the therapeutic potential of LLLT in the management of musculoskeletal pain. However, significant controversy persists in the literature regarding its specific efficacy in cervical pain syndrome, particularly in the acute and subacute phases. (15,16) There is methodological heterogeneity in the available studies regarding application parameters (wavelength, energy density, exposure time), treatment protocols, and control group selection. (17,18)
Additionally, there are few studies evaluating the synergistic effect of LLLT combined with cryotherapy, an intervention widely used in the acute phase for its anti-inflammatory and analgesic effects. (19-21)
It is unknown whether the application of low-level laser therapy combined with cryotherapy is more effective than conventional treatment with NSAIDs and cryotherapy in improving pain intensity and functional capacity in patients with acute and subacute cervical pain syndrome treated in the rehabilitation department of the "Faustino Pérez" Provincial Clinical and Surgical Teaching Hospital in Matanzas.
This study aimed to evaluate the effectiveness of low-level laser treatment in patients with acute and subacute cervical pain syndrome treated at the Faustino Pérez Hospital in Matanzas.
METHODOLOGY
An experimental, longitudinal, and prospective study was conducted in the Rehabilitation Service of the Faustino Pérez Provincial Clinical-Surgical Teaching Hospital from January to December 2024.
The sample consisted of 87 patients diagnosed with acute and subacute cervical pain syndrome, and the sample consisted of 38 patients who consented to participate in the research and met the following criteria:
Inclusion criteria: patients over 20 years of age; neck pain of less than 7 weeks' duration; pain perception, according to the visual analog scale, of 4 or more; cervical osteoarthritis, tension, postural, mechanical, and inflammatory conditions.
Exclusion criteria: symptoms, signs, or history of non-benign diseases; decompensated mental illness; history of severe trauma involving spinal cord involvement; being under a treatment program other than the one under study; and extracervical inflammatory processes. Patients with a history of gastroduodenal ulcer or NSAID intolerance.
Exit criterion: voluntarily. Patients who missed more than 3 treatment sessions.
Patients were randomly assigned to one of the two treatment programs established in the study design.
Group 1 (study): cervical cryotherapy plus localized laser therapy in the rehabilitation department.
Group 2 (control): cervical cryotherapy plus Ibuprofen (400 mg tablet) 1 tablet every 8 hours.
Each patient in the sample underwent a physiotherapy evaluation at the beginning and end of treatment, which included a history, physical examination, and the administration of pain (VAS and Likert test) and disability (NDI) questionnaires.
The visual analog scale represents a line graduated in centimeters from zero to ten, where zero represents the absence of pain and ten represents maximum pain. The Likert test describes pain intensity according to the following five aspects: No pain, mild, bothersome, intense, and unbearable.
The Neck Disability Index (NDI) was self-administered by the patient and consists of 10 items that reflect daily living activities and how they may be influenced by neck pain.
Treatment effectiveness criteria were analyzed by group using the formula:
![]()
The treatment programs consisted of local cryotherapy administered to the cervical region for 10 minutes every 4 hours at home. They differed in that one group received infrared laser therapy using a LaserMed 670 device from TECE, S.A., developed by Cuban companies, for 20 seconds at each point at a dose of 5 J/cm2 around the painful area, maintaining a distance of 2 to 3 cm between the points. The other group received 400 mg of ibuprofen every 8 hours, in both cases as the sole treatment for 10 days.
The results were evaluated as follows:
· Good: Reduction of 4 cm or more on the VAS. Likert test at 1. NDI, no disability.
· Fair: Reduction, difference from initial pain between 3 and 3.9 cm on the VAS. Likert test at 2. NDI with mild disability
· Poor: Continued pain or a difference from initial pain between 2 and 2.9 cm on the VAS. Likert test between 3 and 5. NDI with moderate/severe disability
Taking as a category the coincidence of two of the instruments used.
The data obtained were recorded in collection sheets designed to include the study variables and the results before and after the intervention. This information was subsequently organized into an Excel database and analyzed using SPSS version 11,5. Differences between pre- and post-rehabilitation measurements were evaluated using the Chi-square test (x2), defining a significance level of α = 0,01 and α = 0,05.
The research protocol was approved by the institution's Research Ethics Committee (Minutes No. 4/Agreement No. 2/2024), in compliance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
RESULTS
There was a high incidence of females, and the largest proportion of the total were between the ages of 35 and 49 (13 patients) and 50 and 64 (9 patients). The mean age of the patients was 42,1 years (Table 1).
Table 1. Distribution of patients with neck pain by age and sex
|
Age |
Sex |
||||||
|
Cluster |
Female |
Male |
Total |
||||
|
No. |
% |
No. |
% |
No. |
% |
||
|
20-34 |
I |
2 |
5,3 |
1 |
2,6 |
3 |
7,9 |
|
II |
1 |
2,6 |
2 |
5,3 |
3 |
7,9 |
|
|
35-49 |
I |
8 |
21,0 |
1 |
2,6 |
9 |
23,7 |
|
II |
5 |
13,2 |
2 |
5,3 |
7 |
18,4 |
|
|
50-64 |
I |
5 |
13,2 |
1 |
2,6 |
6 |
15,7 |
|
II |
4 |
10,5 |
1 |
2,6 |
5 |
13,2 |
|
|
+ de 65 |
I |
2 |
5,3 |
1 |
2,6 |
3 |
7,9 |
|
II |
2 |
5,3 |
- |
- |
2 |
5,3 |
|
|
Total |
|
29 |
76,4 |
9 |
23,6 |
38 |
100 |
Source: Data collection form.
Table 2 assesses risk factors and shows that 32 of the 38 patients, or 84,2 %, have poor postural habits, followed by a lack of physical exercise (76,3 %).
Lack of exercise (76,3 %) was another relevant risk factor, cited by some authors as an important factor in triggering pain due to a lack of a strengthened vertebral segment.
Chronic tension (68,4 %) was identified as a triggering factor or as a contributor to the prolongation of the condition, constituting a vicious tension-pain-tension syndrome.
Another factor is occupations with high physical effort, which are associated with neck pain due to repetitive movements, lack of breaks during work, static loads, and sustained postures with the head or arms. Both samples were homogeneous in terms of risk factors, which was statistically significant (χ2 = 0,261, with a degree of freedom of 1, p = 0,576).
Table 2. Distribution according to associated risk factors
|
Risk factors |
Sex |
|||||
|
Female n=29 |
Male n=9 |
Total n = 38 |
||||
|
No. |
% |
No. |
% |
No. |
% |
|
|
Poor postural habits |
25 |
86,2 |
7 |
77,8 |
32 |
84,2 |
|
Lack of physical exercise |
23 |
79,3 |
6 |
66,7 |
29 |
76,3 |
|
Chronic tension |
19 |
65,5 |
7 |
77,8 |
26 |
68,4 |
|
Intense physical exertion at work |
15 |
51,7 |
5 |
55,6 |
20 |
52,6 |
Source: Data collection form.
The difference in pain between the start and end of treatment according to the VAS, as shown in the graph, was significant in 16 patients, representing 76,2 % of those who received laser treatment. Graph 1
Graph 1. Differences in pain according to the VAS for both treatments
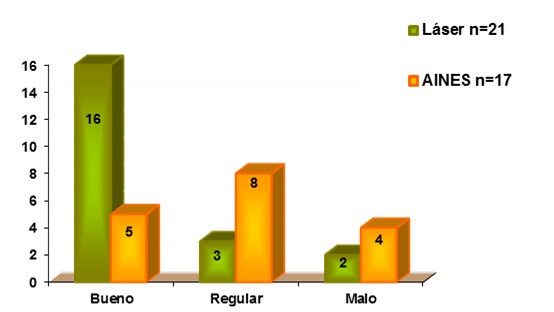
Source: Data collection form.
When these results were compared with the Likert scale also applied before and after treatment (Table 3), the group of patients treated with cryotherapy and low-level laser experienced intense and unbearable pain first, with 52,4 % and 28,6 %, as did the cryotherapy and NSAID group, with 41,2 % and 29,4 %, respectively. The post-treatment results were not the same, as 52,4 % and 23,8 % of patients treated with laser experienced pain-free or mild pain, while those treated with NSAIDs experienced pain-free or mild pain only in 17,7 % and 23,5 %. These findings make the difference statistically significant with a 95 % confidence interval, which could be verified using the Chi-square test (p < 0,05).
Table 3. Pain distribution according to the Likert scale before and after treatment
|
Likert scale |
Laser n = 21 |
NSAIDs n = 17 |
|||||||
|
Before |
After |
Before |
After |
||||||
|
No. |
% |
No. |
% |
No. |
% |
No. |
% |
||
|
No pain |
- |
- |
11 |
52,4 |
- |
- |
3 |
17,7 |
|
|
Mild |
- |
- |
5 |
23,8 |
- |
|
4 |
23,5 |
|
|
Annoying |
4 |
19 |
3 |
14,3 |
5 |
29,4 |
5 |
29,4 |
|
|
Intense |
11 |
52,4 |
2 |
9,5 |
7 |
41,2 |
4 |
23,5 |
|
|
Unbearable |
6 |
28,6 |
- |
- |
5 |
29,4 |
1 |
5,9 |
|
Source: Data collection form.
The relationship of pain with activities of daily living according to the Neck Disability Index (NDI), as shown in Table 4, behaved in the laser group before treatment with 52,4 % of moderate disability, with a mean of 22,9 ± 6,4 SD as well as in the NSAID group with 47,1 %, with a mean of 20,8 ± 4,4 SD. After treatment the predominance in the laser group was 47,6 % of mild disability and no disability in 33,3 %; With a mean of 6,4 ± 4,5 SD, the same trend was not observed in the NSAID group, where the predominance of moderate disability remained at 47,1 % and mild disability at 35,2 %, with a mean of 14,8 ± 3,7 SD.
Table 4. Relationship between pain and disability in activities of daily living according to the Neck Disability Index (NDI) Questionnaire
|
NDI Questionnaire |
Laser n = 21 |
NSAIDs n = 17 |
|||||||
|
Before |
After |
Before |
After |
||||||
|
No. |
% |
No. |
% |
No. |
% |
No. |
% |
||
|
No disability |
- |
|
7 |
33,3 |
1 |
5,9 |
1 |
5,9 |
|
|
Mild disability |
4 |
19 |
10 |
47,6 |
4 |
23,5 |
6 |
35,2 |
|
|
Moderate disability |
11 |
52,4 |
3 |
14,3 |
8 |
47,1 |
8 |
47,1 |
|
|
Severe disability |
5 |
23,8 |
1 |
4,8 |
3 |
17,6 |
2 |
11,8 |
|
|
Complete disability |
1 |
4,8 |
- |
- |
1 |
5,9 |
- |
- |
|
Source: Data collection form. p < 0,05
When comparing the effectiveness of both treatment programs (Table 5), the program that included cryotherapy and laser treatment was found to have a 76,2 % effectiveness rate (52,4 % and 23,8 % of patients evaluated with pain-free or mild pain, respectively), higher than the 70,5 % effectiveness rate obtained with cryotherapy and NSAIDs (17,7 % with pain-free and 23,5 % with mild pain, respectively). Both treatments were proven effective according to the percentages expressed, but in the independent statistical analysis of each method to determine which of the two reported greater effectiveness, it was found that group 1, which included cryotherapy and laser, had greater statistical significance, as verified by the Chi-square test (p < 0,05).
Table 5. Results according to the treatment applied
|
Results |
Treatment applied |
|||
|
Laser Cryotherapy n = 21 |
NSAIDs-cryotherapy n = 17 |
|||
|
No. |
% |
No. |
% |
|
|
Good |
16 |
76,2 |
12 |
70,5 |
|
Average |
5 |
23,8 |
4 |
23,5 |
|
Bad |
- |
- |
1 |
5,8 |
|
Total |
21 |
100 |
17 |
100 |
Source: Data collection form.
DISCUSIÓN
The study conducted at the Faustino Pérez Provincial Clinical and Surgical Teaching Hospital confirmed the effectiveness of low-level laser therapy in the treatment of cervical pain syndrome. Consistent with data from the World Health Organization (2), a greater incidence of cervical pain was observed in women, which is partly attributed to the mechanical origin of cervical pain and the additional burdens women assume in housework, thus increasing their vulnerability.
Bovim G et al. (3) noted that the general population, especially women with poor postural habits and low physical activity, has a higher incidence of cervical pain. Although cautious, they mention that the prevalence of persistent pain after whiplash is comparable to that of chronic cervical pain in the general population. Likewise, Van der Donk et al. (4) associated improper posture, particularly in sedentary occupations such as office workers who use computers, as a significant risk factor for the development of cervical pain.
An important finding of this study was the presence of chronic tension in 68,4 of patients, identified as a triggering and maintaining factor of the pain-tension cycle. This pattern has been reported in the literature as a significant negative factor, also influenced by psychological and social factors, and observed in both working women and homemakers. (3)
Furthermore, occupations that involve intense and repetitive physical exertion, with static postures and a lack of work breaks, are associated with the development of neck pain, particularly in its acute and subacute phases. (8)
During treatment, pain improvement, assessed by the visual analogue scale (VAS) and the Likert scale, was significant. According to experts from the Spanish Network of Back Pain Researchers, for a patient to perceive real relief, a reduction of approximately 30 % of the initial pain intensity is required; Decreases of less than 1,5 points on a scale of 0 to 10 are considered clinically irrelevant. (8,11) In this context, both Touma et al. (8) and the Philadelphia Clinical Evidence Panel (10) recognize the usefulness of NSAIDs in the management of neck pain.
The results of this study are consistent with previous research demonstrating the efficacy of low-level laser in relieving chronic neck pain compared to conventional therapies such as infrared rays, highlighting faster and longer-lasting relief. (12) De Oliveira et al. (13) also reported greater effectiveness of low-level laser, especially when combined with exercise, although they emphasized the lack of studies on its application in the acute and subacute phases, particularly in combination with cryotherapy.
The average number of sessions required to achieve pain relief and improvements in daily activities with cryotherapy and laser was 13.4, lower than the 14,3 days observed with conventional treatments. This is consistent with other studies that have evaluated this modality for neck pain, even in chronic phases. (14,22)
Finally, the improvement in daily activities observed in patients treated with laser and cryotherapy is considered to be supported by a significant reduction in pain—more than 30 %—which allowed most of them to resume activities previously limited by pain.
While the results demonstrate the effectiveness of the rehabilitation program, certain limitations are important to consider. First, the study was conducted at a single center, which may affect the generalizability of the results. Another limitation was the limited follow-up period, which makes it impossible to assess the sustainability of the long-term benefits. Furthermore, consecutive sampling could have introduced some selection bias. Finally, a cost-benefit analysis was not performed to assess the economic feasibility of implementing this program on a larger scale. These limitations suggest the need for future studies with longer follow-up periods to confirm these findings. Despite these limitations, the results provide evidence of the effectiveness of rehabilitation treatment programs in patients with acute and subacute cervical pain syndrome.
CONCLUSIONS
This study confirms the effectiveness of low-level laser treatment in patients with acute and subacute cervical pain syndrome treated at the Faustino Pérez Hospital in Matanzas. Both treatment programs achieved pain relief and improved functional disability; however, the protocol combining cryotherapy with low-level laser demonstrated greater speed and efficacy in symptom reduction. Therefore, the combination of cryotherapy and laser is positioned as a superior therapeutic alternative to conventional cryotherapy-based physiotherapy and the use of NSAIDs for the management of cervical pain syndrome in its acute and subacute phases.
BIBLIOGRAPHIC REFERENCES
1. Mohd Isa IL, Teoh SL, Mohd Nor NH, Mokhtar SA. Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci. 2022 [cited 21/01/2025]; 24(1):208. Available in: https://pubmed.ncbi.nlm.nih.gov/36613651/
2. Organización Mundial de la Salud. Osteoartritis. [Internet] 2023 [cited 21/01/2025]. Available in: https://www.who.int/news-room/fact-sheets/detail/osteoarthritis
3. Bovim G, Schrader H, Sand T. Neck pain in the general population. Spine. [Internet] 1994 [cited 21/01/2025]; 19(12):1307-1309. Available in: https://www.journal.lww.com/spinejournal/abstract/1994/06000
4. Van der Donk J, Schoulten JAS, Passchier J, Romunde LK, Valkenburg HA. The associations of neck pain with radiological abnormalities of the cervical spine and personality traits in a general population. J Rheumatol. [Internet] 1991 [cited 21/01/2025]; 18(12):1884-1889. Available in: https://www.scopus.com/pages/publications/0026344063
5. Westerling D, Jonsson BG. Pain from the neck-shoulder region and sick leave. Scand J Soc Med. [Internet] 1980 [cited 21/01/2025]; 8(3):131-136. Available in: https://www.scopus.com/pages/publications/0019200486
6. Pineda-Moncusí M, Dernie F, Dell'Isola A, Kamps A, Runhaar J, Swain S, et al. Classification of patients with osteoarthritis through clusters of comorbidities using 633,330 individuals from Spain. Rheumatology (Oxford). [Internet] 2023 [cited 21/01/2025]; 62(11):3592-3600. Available in: https://www.sciencedirect.com/science/article/abs/pii/S0211563807744371
7. Adogwa O, Buchowski J, Sielatycki J, Shlykov M, Theologis A, Lin J, et al. Improvements in Neck Pain and Disability Following C1-C2 Posterior Cervical Instrumentation and Fusion for Atlanto-Axial Osteoarthritis. World Neurosurgery. [Internet] 2020 [cited 22/01/2025]; 139:496-500. Available in: https://pubmed.ncbi.nlm.nih.gov/32311554/
8. Touma J, May T, Isaacson A. Cervical Myofascial Pain. StatPearls [Internet]. 2023 [cited 21/01/2025]. Available in: https://www.ncbi.nlm.nih.gov/books/NBK507825/
9. Gross AR, Hoving JL, Haines TA, Goldsmith CH, Kay T, Aker P; Cervical Overview Group. A Cochrane review of manipulation and mobilization for mechanical neck disorders. Spine. [Internet] 2004 [cited 22/01/2025]; 29(15):1541-1548. Available in: https://journals.lww.com/spinejournal/abstract/2004/07150/a_cochrane_review_of_manipulation_and_mobilization.9.aspx
10. Philadelphia Panel Evidence-Based Clinical Practice Guidelines on Selected Rehabilitation Interventions: Overview and Methodology. Phys Ther. [Internet] 2001 [cited 22/01/2025]; 81(9):1629-1640. Available in: https://pubmed.ncbi.nlm.nih.gov/11589641/
11. Medina I, Mirapeix F, Saturno Hernández P, Mantilla Herrador J, Valera Garrido JF, Escalar Reina P, et al. Variabilidad en la valoración del paciente con cervicalgia mecánica en fisioterapia. Un estudio usando protocolos. Fisioterapia. [Internet] 2007 [cited 22/01/2025]; 29:190-195. Available in: https://www.sciencedirect.com/science/article/abs/pii/S0211563807744371
12. Shergill Y, Coté P, Shearer H, Wong JJ, Stupar M, Tibbles A, Cassidy JD. Inter-rater reliability of the Quebec Task Force classification system for recent-onset Whiplash Associated Disorders. J Can Chiropr Assoc. [Internet] 2021 [cited 22/01/2025]; 65(2):186-192. Available in: https://pubmed.ncbi.nlm.nih.gov/34658390/
13. De-Oliveira M, Johnson D, Demchak T, Tomazoni S, Leal-Junior EC. Low-intensity LASER and LED (photobiomodulation therapy) for pain control of the most common musculoskeletal conditions. Eur J Phys Rehabil Med. [Internet] 2022 [cited 22/01/2025]; 58(2):282-289. Available in: https://pubmed.ncbi.nlm.nih.gov/34913330/
14. Childress M, Stuek S. Neck Pain: Initial Evaluation and Management. Am Fam Physician. [Internet] 2020 [cited 22/01/2025]; 1(1):1-7. Available in: https://pubmed.ncbi.nlm.nih.gov/32735440/
15. Nasuk GR, Matos LP, Atum ALB, de Jesus BC, Batista JGC, da Silva GA, et al. Photobiomodulation Therapy Reduces Oxidative Stress and Inflammation to Alleviate the Cardiotoxic Effects of Doxorubicin in Human Stem Cell-Derived Ventricular Cardiomyocytes. Biomedicines. [Internet] 2025 [cited 22/01/2025]; 13(7):1781. Available in: https://pubmed.ncbi.nlm.nih.gov/40722850/
16. Tehrani M, Nazary-Moghadam S, Zeinalzadeh A, Moradi A, Mehrad-Majd H, Sahebalam M. Efficacy of low-level laser therapy on pain, disability, pressure pain threshold, and range of motion in patients with myofascial neck pain syndrome: a systematic review and meta-analysis of randomized controlled trials. Lasers Med Sci. [Internet] 2022 [cited 22/01/2025]; 37(6):3333-3341. Available in: https://pubmed.ncbi.nlm.nih.gov/35962884/
17. Rola P, Wlodarczk S, Lesiak M, Doroszko A, Wlodarczk A. Cambios en la biología celular bajo la influencia de la terapia láser de baja intensidad. Photonics. [Internet] 2022 [cited 22/01/2025]; 9(7):502. Available in: https://www.mdpi.com/2304-6732/9/7/502
18. Makin J, Watson L, Pouliopoulou DV, et al. Effectiveness and safety of manual therapy when compared with oral pain medications in patients with neck pain: a systematic review and meta-analysis. BMC Sports Sci Med Rehabil. [Internet] 2024 [cited 21/01/2025];16(1):86. Available in: https://pubmed.ncbi.nlm.nih.gov/38627846/
19. Alayat MSM, et al. Efficacy of low-level laser therapy on cervical myofascial pain: a systematic review and meta-analysis. Lasers Med Sci. [Internet] 2023 [cited 22/01/2025]; 38(1):1-14. Available in: https://pubmed.ncbi.nlm.nih.gov/35962884/
20. De-Souza TO, et al. Photobiomodulation therapy for chronic cervical pain: a systematic review with network meta-analysis. J Clin Med. [Internet] 2022 [cited 22/01/2025]; 11(15):4519. Available in: https://pubmed.ncbi.nlm.nih.gov/34767117/
21. Flynn DM. Chronic Musculoskeletal Pain: Nonpharmacologic, Noninvasive Treatments. Am Fam Physician. [Internet] 2020 [cited 22/01/2025]; 102(8):465-477. Available in: https://pubmed.ncbi.nlm.nih.gov/33064421/
22. Montemuiño-Muñiz A. Mecanismos de acción y efectos de la crioterapia en la fase precoz de la respuesta inflamatoria secundaria a lesiones de partes blandas: revisión sistemática [Trabajo de Fin de Grado]. Universidade da Coruña; [Internet] 2018 [cited 22/01/2025]. Available in: https://ruc.udc.es/entities/publication/6e89be28-132a-439e-b7cc-5783fc6056d3
AUTHORSHIP STATEMENT
LMHF: conceptualization, data curation, funding acquisition, research, methodology, project administration, resources, software, supervision, validation, visualization, draft writing, writing, reviewing, and editing the final manuscript.
JBPB: conceptualization, data curation, research, methodology, supervision, validation, visualization.
GGP: conceptualization, data curation, research, methodology, supervision, validation, visualization.
ITHH: conceptualization, data curation, research, methodology, supervision, validation, visualization.
NMD: conceptualization, data curation, research, methodology, supervision, validation, visualization.
MDR: conceptualization, data curation, research, methodology, supervision, validation, visualization.
CONFLICTS OF INTEREST
The authors declare that there is no conflict of interest.
SOURCES OF FUNDING
The authors declare that they received no funding for the development of this research.