CASE PRESENTATION
Green nail syndrome due to Pseudomonas aeruginosa associated with acrylic nails: case report
Síndrome de la uña verde por Pseudomona aeruginosa asociado a uñas acrílicas: presentación de caso
Alvaro Rojas Mora 1*, https://orcid.org/0000-0001-6805-5364
Aylet Pérez López 1, https://orcid.org/0000-0003-4629-9995
Tania Torriente Esquivel 1, https://orcid.org/0000-0001-9943-5300
Graciela Fundora Guerra 1, https://orcid.org/0009-0000-9273-0403
1 Calixto García General University Hospital. Havana. Cuba
* Corresponding author: alvarorojasmorapiel@gmail.com
Received: 05/01/2026
Accepted: 15/03/2026
Published: 18/03/2026
How to cite this article: Rojas-Mora A, Pérez-López A, Torriente-Esquivel T, Fundora-Guerra G. Green nail syndrome due to Pseudomonas aeruginosa associated with acrylic nails: case report. MedEst. [Internet]. 2026 [cited access date]; 6:e506. Available in: https://revmedest.sld.cu/index.php/medest/article/view/506
ABSTRACT
Introduction: Green nail syndrome, or chloronychia, is an infectious onychopathy characterized by green discoloration of the nail plate, predominantly caused by Pseudomonas aeruginosa. It is classically associated with occupational exposure to moisture, but cosmetic nail procedures such as acrylic nails have been recognized as an emerging risk factor.
Objective: To report a clinical case of extensive chloronychia secondary to acrylic nail application, highlighting its atypical non-inflammatory presentation, the usefulness of onychoscopy in diagnosis, and the effectiveness of combined therapeutic management.
Case presentation: A 26-year-old female patient presented with greenish discoloration of the nail of her left first toe, which began 15 days after acrylic nail application. Physical examination revealed extensive chloronychia with distal onycholysis, but no paronychia. Onychoscopy revealed a diffuse green pattern with subungual debris. Culture confirmed ciprofloxacin-sensitive Pseudomonas aeruginosa. A combination of hygiene measures, 1% acetic acid soaks, topical gentamicin, and oral ciprofloxacin was initiated. Complete resolution of the pigmentation was observed within one month, with definitive clinical cure confirmed at three months.
Conclusions: This case highlights that chloronychia can present extensively but not be inflammatory; cosmetic nail procedures are a relevant and preventable risk factor; onychoscopy is a key diagnostic tool; in cases with extensive involvement, a combined therapeutic approach (topical and systemic) can ensure rapid and lasting resolution.
Keywords: Green nail syndrome; Pseudomonas aeruginosa.
RESUMEN
Introducción: El síndrome de la uña verde o cloroniquia es una onicopatía infecciosa caracterizada por la decoloración verde de la lámina ungueal, causada predominantemente por Pseudomona aeruginosa. Se asocia de forma clásica a exposición ocupacional a humedad, pero los procedimientos cosméticos ungueales como las uñas acrílicas se han reconocido como un factor de riesgo emergente.
Objetivo: Reportar un caso clínico de cloroniquia extensa secundaria a la colocación de uñas acrílicas, destacando su presentación atípica no inflamatoria, la utilidad de la onicoscopia en el diagnóstico y la eficacia de un manejo terapéutico combinado.
Presentación del caso: Paciente femenina de 26 años, acude por coloración verdosa de la uña del 1er dedo del pie izquierdo, iniciada 15 días tras la colocación de uñas acrílicas. Al examen físico presentaba cloroniquia extensa, con onicólisis latero distal, pero ausencia de paroniquia. La onicoscopia mostró patrón verde difuso con detrito subungueal, el cultivo confirmó Pseudomona aeruginosa sensible a ciprofloxacino. Se instauró tratamiento combinado con medidas higiénicas, fomentos de ácido acético al 1 %, gentamicina tópica y ciprofloxacino oral. Se observó resolución completa de la pigmentación al mes, confirmándose curación clínica definitiva a los 3 meses.
Conclusiones: Este caso destaca que la cloroniquia puede presentarse de forma extensa pero no inflamatoria; los procedimientos cosméticos ungueales son un factor de riesgo relevante y prevenible; la onicoscopia es una herramienta clave para el diagnóstico; en casos con afectación extensa, un abordaje terapéutico combinado (tópico y sistémico) puede asegurar una resolución rápida y duradera.
Palabras clave: Síndrome de la uña verde; Pseudomona aeruginosa.
INTRODUCTION
Green discoloration of the nail plate is a characteristic clinical sign of infection, with green nail syndrome, also known as chloronychia or Goldman-Fox syndrome, being its main manifestation. (1) This infectious onychopathy is characterized by a blue-green pigmentation of the nail, secondary to colonization by Pseudomonas aeruginosa, an opportunistic gram-negative bacillus that produces pyocyanin and pyoverdine, pigments responsible for the characteristic staining. (2)
Classically described in occupational settings with chronic exposure to moisture, chloronychia has undergone a recent epidemiological shift. Cosmetic nail procedures, particularly acrylic nails, are emerging as a frequently underestimated preventable risk factor in clinical practice. (3,4) The classic triad of green discoloration, onycholysis, and paronychia is not always present in its entirety; extensive atypical forms with minimal inflammatory response exist, posing a diagnostic challenge. (4)
The diagnosis is based on the correlation of clinical, onychoscopic, and microbiological findings. Dermatoscopy allows for the identification of characteristic pigmentary patterns, while culture confirms the bacterial species and its antimicrobial susceptibility. (2) Treatment varies according to the extent of the infection, ranging from hygiene measures and topical therapy to systemic antibiotic therapy in extensive or recalcitrant cases. (1,4)
The objective of this study is to report a case of extensive chloronychia secondary to acrylic nails in a young patient, highlighting its atypical presentation, the diagnostic value of onychoscopy, and the effectiveness of a combined approach.
This case illustrates the importance of investigating cosmetic habits in patients with green nail syndrome and contributes to characterizing the atypical clinical forms of this emerging infection.
CASE PRESENTATION
A 26-year-old female patient, previously healthy, with no relevant medical or surgical history, and no known drug allergies. She presented to the dermatology outpatient clinic at the Calixto García General University Hospital (Havana, Cuba) with a 15-day history of greenish discoloration of the toenail on her left big toe. The discoloration began two weeks after the application of acrylic artificial nails to both feet, a procedure performed at a beauty salon. The patient denied pain, itching, discharge, previous trauma, or occupational exposure to chronic moisture.
Dermatological physical examination:
Nail apparatus of the left big toe: extensive chloronychia affecting approximately 90% of the nail plate surface, with homogeneous blue-green pigmentation. Distal and lateral onycholysis, affecting approximately 40% of the nail surface. No erythema, edema, pain on palpation, or signs of suppuration were present in the nail matrix or periungual folds (Figure 1). No masses were palpated, and no peripheral vascular abnormalities were observed. The remaining fingernails and toenails appeared normal.
Additional studies
Onychoscopy: Diffuse and confluent green pigmentation pattern, with shades ranging from light to dark green, consistent with pyocyanin production by P. aeruginosa. Abundant subungual debris and well-defined distal and lateral onycholysis were present (Figure 2).
Microbiology: Bacterial culture of subungual material obtained from the onycholysis area, plated on blood agar and MacConkey agar, revealed growth of Pseudomonas aeruginosa sensitive to ciprofloxacin, gentamicin, and amikacin, and resistant to ceftazidime. Direct examination with 10% potassium hydroxide and mycological culture were negative for fungi.
Diagnosis: Green nail syndrome (chloronychia) due to Pseudomonas aeruginosa. ICD-11: EA10.2 (nail and nail bed infection)
/1C1G.0 (Pseudomonas infection)

Figure 1: Extensive chloronychia, affecting more than 90% of the nail surface, associated with predominantly distal onycholysis.
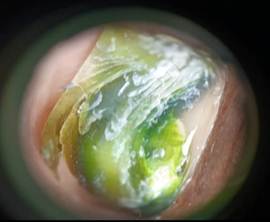
Figure 2: Diffuse and confluent green pigmentation pattern, with areas of variable intensity, from light to dark green tones, abundant subungual debris and lateral and distal onycholysis.
Treatment and evolution
Multimodal therapeutic management was implemented:
General measures: Immediate removal of the acrylic nail; instruction to keep the area dry, avoid occlusive footwear and mechanical trauma; straight cut of the nail; daily change of cotton socks; and education on not sharing pedicure instruments.
Topical treatment: Compresses with 1% acetic acid solution (extemporaneous preparation: 1 mL of glacial acetic acid in 99 mL of distilled water), applied for 15 minutes, twice a day, followed by application of 0.1% gentamicin sulfate cream (gentamicin 1 mg/g) under the free edge of the affected nail.
Systemic treatment: Ciprofloxacin 500 mg orally every 12 hours (1 g/day) for 14 days, adjusted according to normal renal function.
Follow-up:
Three weeks after treatment, complete resolution of the green pigmentation and a significant reduction in onycholysis (approximately 10% of the surface area) were observed.
At three months, definitive clinical cure was confirmed, with complete restoration of the normal color and architecture of the nail plate, without evidence of recurrence or aesthetic or functional sequelae.
Informed consent: Written informed consent was obtained from the patient for the publication of this clinical case, guaranteeing the confidentiality of her identity by removing identifiable data.
DISCUSSION
This case illustrates the epidemiological shift in green nail syndrome over the last decade. Classically, this condition was associated with professions involving chronic exposure to moisture. (1,3) However, in our patient, a young woman with no high-risk occupation, the infection developed as a complication of a cosmetic procedure. The application of acrylic nails creates an occluded subungual microenvironment that promotes local moisture and carries a risk of microtrauma during application and subsequent detachment. (4,6) The direct temporal association of 15 days between the procedure and the onset of symptoms reinforces the hypothesis of coincidence, coinciding with the case reported by Galeas-Calleja and Raudales-Moncada in Mexico (1) and differing from other series that report longer latency periods. (7) Consequently, a thorough history of cosmetic habits emerges as an essential element in the evaluation of patients with green nail syndrome, particularly in young women. (4,11)
A particularly illustrative finding in this case was the extensive involvement of the nail plate (more than 90% of its surface) in the absence of paronychia. This clinical presentation deviates from the classic triad described in the literature (3) and suggests that, in infections maintained under occlusive conditions, such as those found under artificial nails, the tissue inflammatory response may be attenuated. (4) In this regard, Hasbún (4), in an updated review of the syndrome during the COVID-19 pandemic, had already noted this clinical variability, attributing it to the opportunistic nature of P. aeruginosa and to local factors capable of modulating the expression of its virulence. The absence of pain and erythema in the patient presented may have contributed to the delay in seeking medical attention (15 days of evolution), which underscores the importance of educating women who wear artificial nails about the warning signs.
Onychoscopy was a first-line diagnostic tool in this case. The diffuse and confluent green pigmentation pattern, with tonal variations from light to dark green, is highly suggestive of pyocyanin production by P. aeruginosa. (2) Maeda et al. (2), in their review of green nails, emphasize that this finding allows differentiation of chloronychia from pigmented onychomycosis caused by Aspergillus or Fusarium, where the pattern is usually more focal or presents longitudinal striations. In the patient presented, onychoscopy guided the etiological diagnosis before the microbiological results were available, allowing for early initiation of targeted treatment. Its use is especially relevant in contexts with limited access to cultures or when rapid confirmation is required. (2,9)
The management implemented—a combination of hygiene measures, topical therapy with acetic acid and gentamicin, plus oral ciprofloxacin—was justified by the extent of the infection. While the literature suggests that topical therapy is sufficient in most cases, there is a consensus that extensive involvement of the nail plate constitutes a valid criterion for initial systemic antibiotic therapy. (1,4,6) Carhart and Espinosa (6) reported resolution with oral ciprofloxacin in a similar case of significant extension, although associated with paronychia. Our case provides further evidence that the extent of the infection, regardless of periungual inflammation, may indicate combined management to ensure rapid resolution and prevent chronicity.
The choice of ciprofloxacin was based on the antibiogram, but also on its excellent nail tissue penetration and its safety profile in young adults. (6,7) One percent acetic acid, for its part, acts by acidifying the subungual environment, inhibiting the growth of P. aeruginosa, which prefers an alkaline pH, and facilitating the penetration of the topical antibiotic. (1,4) Complete resolution within three weeks and definitive healing within three months, without recurrence, validate this multimodal strategy.
This case underscores that cosmetic nail procedures represent a preventable risk factor. Educating beauty professionals on sterilization techniques, avoiding microtrauma, and recognizing warning signs for medical referral could reduce the incidence of this infection. (1,5) It also highlights the need for dermatologists to explicitly include the use of artificial nails in the medical history of patients with onychopathies, regardless of the clinical presentation.
As an inherent limitation of case reports, generalizing these findings requires caution. Molecular studies were not performed to characterize the isolated strain, nor were biochemical parameters of the subungual environment measured that could explain the absence of an inflammatory response. Prospective studies with a larger number of patients would allow for the establishment of more precise criteria for indicating systemic treatment based on the extent of the infection, independent of the presence of paronychia.
CONCLUSIONS
Green nail syndrome can present with extensive involvement of the nail plate in the absence of periungual inflammatory signs, particularly when the infection is maintained under occlusion by artificial nails. Cosmetic nail procedures constitute a preventable risk factor that should be actively investigated in the medical history of patients with greenish onychodyschromia, regardless of the presence of paronychia. Onychoscopy allows for the identification of characteristic pigmentary patterns that guide the early etiological diagnosis, complementing the microbiological gold standard. In cases of massive involvement, combined topical and systemic treatment ensures rapid and lasting resolution, constituting an effective strategy against atypical clinical forms.
BIBLIOGRAPHIC REFERENCES
1. Galeas-Calleja NI, Raudales-Moncada JC. Síndrome de uña verde secundario a colocación de uñas acrílicas: reporte de caso. Rev Mex Med Fam. 2025 Mar;12(1):30-4. DOI: 10.24875/rmf.24000196
2.Sierra-Maeda KY, López-Segundo S, Vega DC, Juárez-Durán ER, Arenas R. Síndrome de las uñas verdes: una revisión. Dermatol CMQ [Internet]. 2022;20(1):78-85. [cited 04/01/2026]. Available in: https://dermatologia.sld.cu/index.php/dermatologia/article/view/112
3.Schwartz RA, Reynoso-Vásquez N, Kapila R. Cloroniquia: el síndrome de Goldman-Fox: implicaciones para pacientes y profesionales sanitarios. Indian J Dermatol. 2020 Jan-Feb;65(1):1-4. DOI: 10.4103/ijd.IJD_277_19
4.Hasbún ZC, Cruz CR. Síndrome de la uña verde: revisión actualizada en una patología emergente en la era de COVID-19. Bol Micol. 2021;36(2):5-11. DOI: 10.22370/bolmicol.2021.36.2.3043
5.Mahajan M, Mahajan BB. Decoloración verdosa causada por extensiones de uñas de gel que simula una infección por Pseudomonas aeruginosa: ¿Vale la pena arriesgarse por la belleza?: informe de un caso. CosmoDerma. 2024;4:121. DOI: 10.25259/CSDM_135_2024
6.Carhart P, Espinosa J, Lucerna A. A case of green nail syndrome diagnosed in the emergency department. Cureus. 2024 Mar 27;16(3):e57032. DOI: 10.7759/cureus.57032
7.Geizhals S, Lipner SR. Retrospective case series on risk factors, diagnosis and treatment of Pseudomonas aeruginosa nail infections. Am J Clin Dermatol. 2020 Apr;21(2):297-302. DOI: 10.1007/s40257-019-00476-0
8.Nakamura T, Yamauchi M, Sonoda S, Aharen D, Ikemura M, Kohagura K, et al. Green nails, red alert: an unusual exit site infection presentation. Perit Dial Int. 2024 Sep;44(5):397-8. DOI: 10.1177/08968608241234529
9.Lee H, Mun JH, Cho S, Park H. Clinical analysis of Pseudomonas aeruginosa-positive and -negative green nail syndrome cases: a single center retrospective analysis. J Dermatol. 2021 Jul;48(7):1073-6. DOI: 10.1111/1346-8138.15832
10.Hur K, Cho S. Chloronychia caused by Pseudomonas oryzihabitans infection. JAAD Case Rep. 2020 Sep;6(9):918-20. DOI: 10.1016/j.jdcr.2020.07.040
11.Dominique WT, Obasi E, Sidhu S. Chloronychia: green nail syndrome caused by Pseudomonas aeruginosa in a younger patient. Cureus. 2025 May 3;17(5):e83382. DOI: 10.7759/cureus.83382
12.Heymann WR. Appending the appendages: new perspectives on Netherton syndrome and green nail syndrome. J Am Acad Dermatol. 2020;83:735-6. DOI: 10.1016/j.jaad.2020.06.087
13.Spernovasilis N, Psichogiou M, Poulakou G. Skin manifestations of Pseudomonas aeruginosa infections. Curr Opin Infect Dis. 2021;34:72-9. DOI: 10.1097/QCO.0000000000000717
14.Perz C, Swink SM, Khurana M. Green nail syndrome in a teenager. J Osteopath Med. 2024;124(3):137-8. DOI: 10.1515/jom-2023-0187
15.Ohn J, Yu DA, Park H, Cho S, Mun JH. Green nail syndrome: analysis of its association with onychomycosis. J Am Acad Dermatol. 2020;83(3):940-2. DOI: 10.1016/j.jaad.2020.01.040
AUTHORSHIP CONTRIBUTION
ARM: Conceptualization, research, data curation, methodology, visualization, drafting of the original manuscript, and revision and editing of the final manuscript.
ALP: Conceptualization, research, and supervision.
TRE: Conceptualization, research, and supervision.
GFG: Conceptualization, research, and supervision.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
FUNDING SOURCES
The authors received no funding for the development of this article.
USE OF ARTIFICIAL INTELLIGENCE
The authors declare that no artificial intelligence was used in the writing of this manuscript.